Pertussis is one of those diseases that can make a vaccination system look weaker than it is. Parents hear that vaccinated teenagers still get whooping cough, public-health departments keep reporting periodic spikes, and the easiest conclusion writes itself: the vaccine must have stopped working. The evidence says something narrower and more interesting.[1][2][3]
The modern acellular pertussis vaccines still do real work. CDC's current efficacy summary says children who complete the 5-dose DTaP series are protected at about 98% in the year after the last dose and about 71% five years later; for adolescent Tdap, protection is about 73% in the first year and about 34% by year four.[1] Maternal Tdap during pregnancy also prevents about 78% of pertussis cases in infants younger than two months and about 90% of hospitalizations in that age group.[1] Those are not failure numbers. They are boundary numbers.
The boundary is the subject here. In high-income countries that switched from whole-cell to acellular vaccines, pertussis control became less about one clean wall against infection and more about a moving balance: strong early protection against severe disease, weaker durability, and much less certainty that the vaccine will shut down nasal carriage and onward spread.[1][2][4][5][6] Once those layers are separated, the resurgence story stops looking like a simple betrayal by one product and starts looking like an immunology trade.
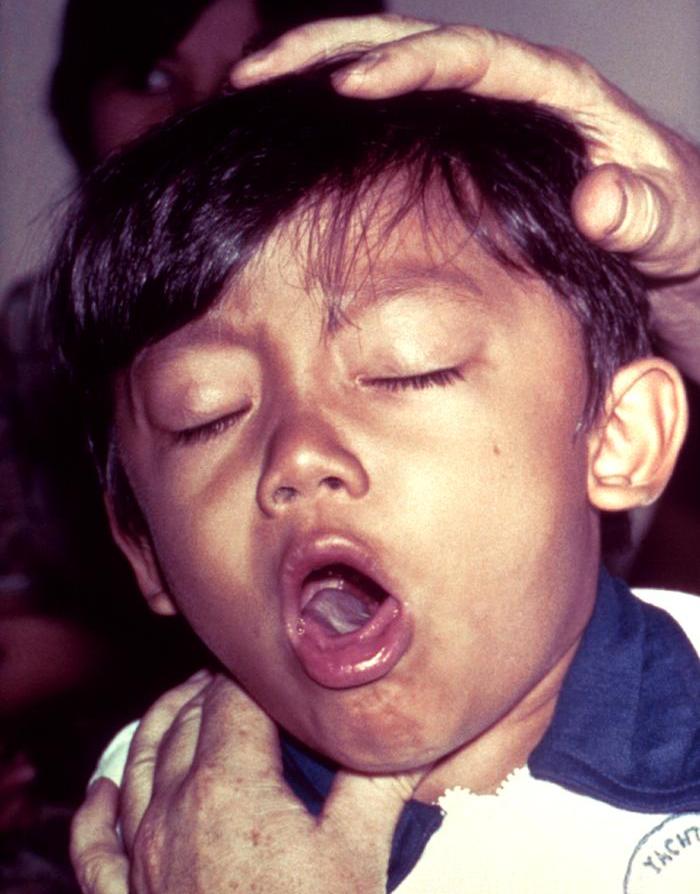
Image context: the cover uses a real CDC clinical photograph of a child with pertussis, sourced via Wikimedia Commons. That matters because the article is about why the system still struggles with circulation even after decades of vaccination, and the right visual anchor is the illness itself rather than an abstract syringe icon.[7]
Timeline anchors before the mechanism
- Late 1940s through the 1990s: the United States relied on combined diphtheria-tetanus-whole-cell pertussis vaccination; reported pertussis cases fell dramatically after whole-cell vaccine entered routine use.[2]
- 1997: CDC's ACIP had moved to a fully recommended 5-dose childhood DTaP series after acellular products replaced DTP in the 1990s because of reactogenicity concerns around the whole-cell component.[2]
- 2005: ACIP recommended a single adolescent and adult Tdap dose, extending the acellular strategy beyond early childhood.[2]
- 2012: ACIP recommended Tdap during each pregnancy to protect infants during the first vulnerable weeks of life.[2]
- 2014: California reported 9,935 pertussis cases by November 26, with incidence peaking at 137.8 cases per 100,000 among 15-year-olds; among adolescents aged 14-16, the median time since prior Tdap was 3 years.[3]
- 2025-2026: CDC's public guidance still describes waning immunity as a key reason pertussis keeps resurfacing and still emphasizes pregnancy vaccination because severe disease remains concentrated in infants too young to be fully vaccinated.[1]
Those dates matter because they show the shape of the trade. Reactogenicity fell. Scheduling became cleaner. Infant and childhood protection remained meaningful. But the immune profile of the program also changed.
1. The acellular switch solved a real problem and created a different one
Whole-cell pertussis vaccines were effective, but they were also more reactogenic. ACIP's historical summary is explicit: DTP was commonly associated with local adverse events and less commonly with serious adverse events, and safety concerns around the whole-cell component drove development and replacement by acellular vaccines in the 1990s.[2] That context matters because it keeps the story honest. Public-health programs did not make an irrational downgrade. They accepted a narrower vaccine design because tolerability and confidence mattered too.
That narrower design still protects against disease. The first thing to avoid, then, is the lazy claim that acellular pertussis vaccine "doesn't work." It clearly does work against the outcome families and clinicians fear most: severe symptomatic infection, especially in early life when the schedule is followed and when maternal Tdap is used to cover the newborn window.[1][2]
The problem is that protection against clinical disease is not the same as durable control of circulation. A program can continue to blunt hospitalizations and infant deaths while doing a less complete job of preventing infection in the upper airway, especially years after the last dose. That is why pertussis can feel paradoxical in vaccinated societies: the vaccines continue to matter profoundly, but the bacteria also keep finding room to move.[1][2][3][4]
2. Waning is not just "antibodies fall"; it begins with the kind of immune memory that gets primed
The 2017 review on mucosal immunity and pertussis resurgence makes the broad epidemiologic point first. U.S. incidence had been rising slowly since the 1970s, but the pace "accelerated sharply" after acellular vaccines replaced whole-cell vaccines in the late 1990s; similar patterns appeared in the United Kingdom, Australia, Ireland, and elsewhere after the same switch.[4] The authors argue that short duration of protection and bacterial adaptation matter, but they are not the whole story.[4]
The deeper mechanism line is immunologic imprinting. In the 2019 study on tissue-resident memory, the authors state the problem plainly: protective immunity wanes rapidly after acellular vaccination, and acellular vaccines do not prevent nasal colonization or transmission in baboons.[5] In their mouse work, whole-cell vaccination protected against lung and nasal colonization, whereas acellular vaccination failed to protect in the nose, and the stronger protection tracked with respiratory TRM cells that secreted IL-17 and IFN-gamma.[5]
That distinction helps explain why "waning" in pertussis is not merely a timer running out on serum antibody levels. The issue is also anatomical. If immune memory in the respiratory tract is weaker, infection can re-establish itself in the nose and nasopharynx more easily, even when the vaccinated person remains partly protected against the more dramatic features of disease.[4][5]
The newest mechanistic mouse paper, published in 2025, sharpens the same argument rather than replacing it. The authors report that current alum-adjuvanted acellular vaccines protect against severe pertussis disease but fail to prevent nasal infection, fail to generate respiratory TRM cells, and instead induce regulatory T-cell signatures linked partly to IL-10; when IL-10 signaling was blocked, or when a stronger adjuvant was paired with nasal delivery, bacterial clearance improved.[6] That is not a direct human policy trial. It is still a useful mechanistic clue: the missing layer is not simply "more booster enthusiasm." The missing layer is respiratory immunity.
3. Once the nose remains partly available, the schedule can protect individuals better than it controls circulation
This is the point where the apparent contradiction resolves. If a vaccine keeps many people from getting the worst version of pertussis but does a weaker job of blocking nasal carriage, the system can still accumulate enough transmission to produce outbreaks every few years.[1][3][4][5]
California's 2014 epidemic is a clean field example. The state reported high disease burden among infants, but incidence was also strikingly high among older children and adolescents, especially the 14-16 cohort that had grown up entirely on acellular products.[3] Among vaccinated adolescents in that age band with complete data, 87% had previously received the Tdap booster, and the median time since that dose was 3 years.[3] That pattern does not mean Tdap was worthless. It means the protection profile had become porous on the time scale that matters for school-age transmission.[1][3]
CDC's current vaccine page gives the same story in shorter form. Protection after Tdap is meaningful in year one and much thinner by year four.[1] That makes pertussis different from the fantasy version of vaccination in which one shot closes the door for a decade and herd effects remain mechanically strong. In pertussis, the schedule increasingly looks like a disease-modification system with incomplete transmission control, especially once several years have passed and exposure keeps cycling through households and schools.[1][3][4]
4. The most dangerous misunderstanding is to read this as an argument against using the current vaccines
The right conclusion is almost the opposite. Because the present vaccines are better at reducing severe disease than at sterilizing transmission, the system has to keep its focus on where severity concentrates: very young infants.[1][2][3] California's 2014 report makes that visible. Among hospitalized pertussis cases with available data, 79% were infants younger than twelve months, and severe disease remained clustered in babies too young to have completed their own vaccination series.[3]
That is why maternal Tdap remains such a central recommendation. It is not a cosmetic add-on. It is the part of the schedule that reaches into the gap before the infant can rely on a personal series.[1][2][3] Likewise, the fact that acellular vaccines do not fully solve carriage is a reason to improve vaccine design and delivery, not a reason to abandon the program that still prevents a large amount of severe disease.
CDC's provider guidance is careful on exactly this point. The agency lists several reasons for modern resurgence: improved diagnosis, better reporting, more circulation, and waning immunity, while also reminding readers that pertussis affects far fewer people today than before widespread vaccination in the 1940s.[1] The sober reading is therefore two-layered. The old vaccines reduced incidence dramatically. The newer acellular regime preserved safety and much of the clinical benefit, but it also left a larger mucosal and durability gap than public intuition expected.[1][2][4][5][6]
5. What would a better pertussis strategy have to change?
The recent literature points in one direction again and again: future progress probably depends on building better respiratory immunity rather than only repeating the current logic harder.[4][5][6] That could mean different adjuvants, different antigen combinations, or different routes such as nasal delivery. It could also mean admitting that the core benchmark should not be severe disease alone if public-health goals include reducing carriage and household spread.
For now, the best explanation of pertussis resurgence is not that modern vaccines failed to do anything useful. It is that they succeeded in a narrower lane than the public imagined. Acellular pertussis vaccines are good enough to blunt a great deal of severe illness, especially when pregnancy vaccination protects infants at the start of life. They are weaker at generating the kind of durable, mucosal, transmission-disrupting immunity that makes circulation collapse. Pertussis keeps returning on schedule because the schedule still leaves the nose partly open.[1][2][3][4][5][6]
Sources
- Centers for Disease Control and Prevention, "Diphtheria, Tetanus, and Pertussis (Whooping Cough) Vaccination: Information for Health Care Providers" - current CDC efficacy, waning, and maternal-pregnancy protection summary.
- CDC ACIP / MMWR, "Prevention of Pertussis, Tetanus, and Diphtheria with Vaccines in the United States" - historical shift from whole-cell DTP to acellular DTaP/Tdap, schedule milestones, and epidemiologic framing.
- Winter K et al., "Pertussis Epidemic - California, 2014" (MMWR, 2014) - infant severity, adolescent 14-16 incidence pattern, and the three-year median since prior Tdap in the high-incidence cohort.
- Gill CJ, Rohani P, Thea DM. "The relationship between mucosal immunity, nasopharyngeal carriage, asymptomatic transmission and the resurgence of Bordetella pertussis" - synthesis linking acellular transition, delayed incidence rise, and the missing mucosal-immunity layer.
- Wilk MM et al. "Immunization with whole cell but not acellular pertussis vaccines primes CD4 TRM cells that sustain protective immunity against nasal colonization with Bordetella pertussis" - mechanistic study on respiratory tissue-resident memory and nasal-colonization control.
- Ni Chasaide C et al. "Acellular Pertussis Vaccines Induce CD8+ and CD4+ Regulatory T Cells That Suppress Protective Tissue-Resident Memory CD4+ T Cells, in Part via IL-10" - 2025 mouse study on regulatory T-cell signatures, IL-10, and intranasal rescue strategies.
- Wikimedia Commons, "File:Pertussis.jpg" - CDC Public Health Image Library source page for the lead clinical photograph used in this article.