Rh disease used to arrive in the nursery as a family shock. A mother who looked healthy could deliver a jaundiced, anemic, or hydropic infant, and the logic would only become fully visible afterward: fetal red cells had entered her circulation in an earlier pregnancy, she had become sensitized, and the next Rh-positive fetus inherited the cost.[1][2] What changed after 1968 was not that obstetrics discovered one dramatic rescue. It discovered a schedule.[2][3]
That schedule is the real subject here. Once RhoGAM entered routine use, the center of gravity moved away from exchange transfusion and toward prevention by blood typing, antibody screening, gestational timing, and a postpartum deadline.[1][3][4] The disease did not vanish, and severe hemolytic disease of the fetus and newborn still exists. But the ordinary governing question changed from "Can we save this baby after the immune attack has already happened?" to "Did the system recognize an Rh-negative pregnancy early enough, and did it hit the prophylaxis window?"[2][3]
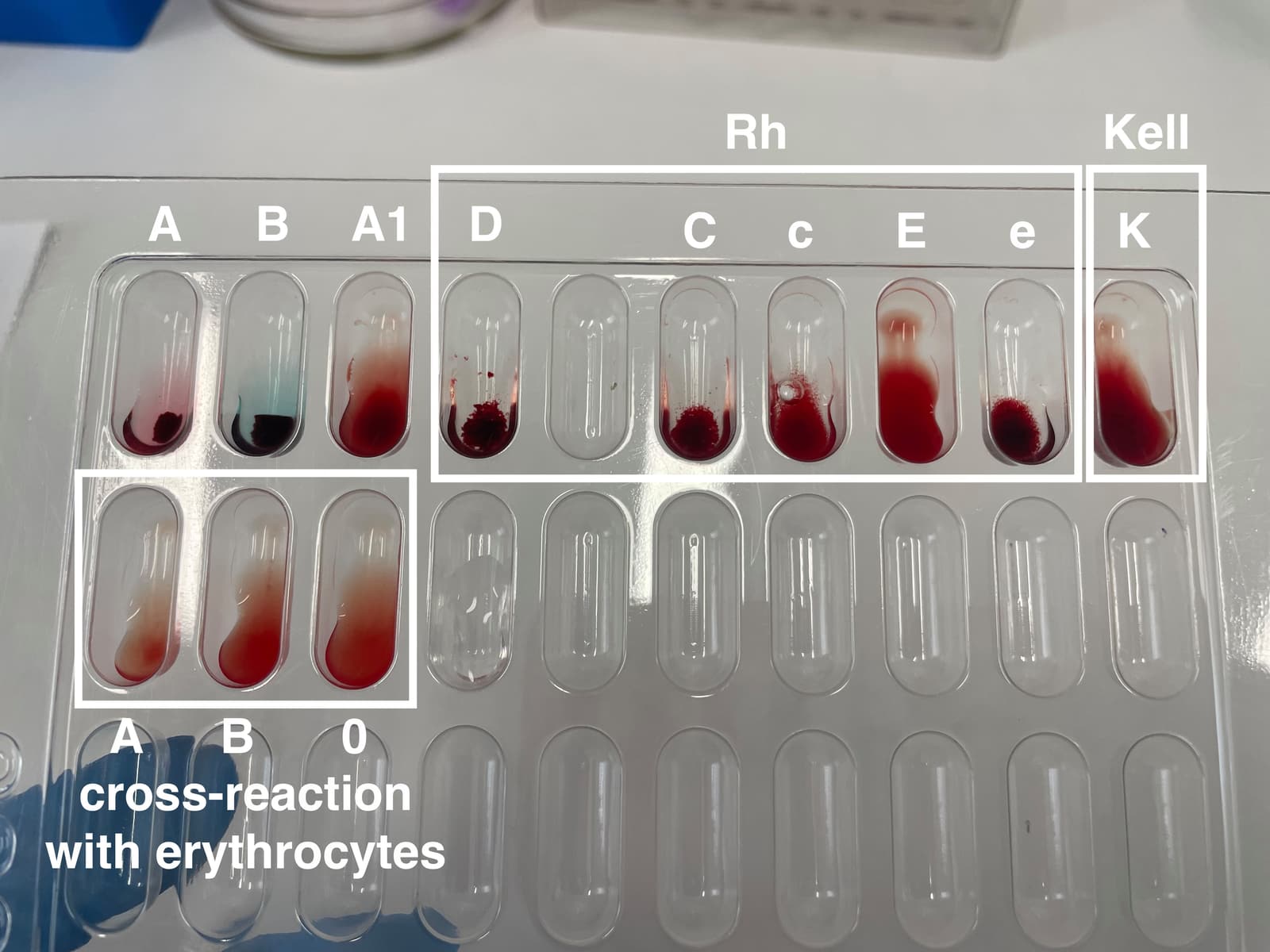
Image context: the cover uses a real clinical photograph of blood-group typing. That is the right visual here because the historical pivot in Rh disease was administrative and laboratory-based as much as therapeutic. Once typing and prophylaxis became routine, the decisive action often happened in the clinic and the blood bank before the nursery ever saw a crisis.[7]
Timeline anchors before the mechanism
- 1932: Louis K. Diamond described erythroblastosis fetalis as a recognizable newborn blood disorder, establishing the syndrome before the Rh mechanism was fully worked out.[2]
- Mid-20th century: Rh disease became a major cause of fetal and neonatal morbidity and mortality in industrial maternity care, especially across later pregnancies after maternal sensitization.[1][6]
- 1968: RhoGAM received initial U.S. approval, creating the first standardized anti-D prophylaxis pathway for unsensitized Rh-negative mothers.[3][6]
- 1970 to 1979: a U.S. public-health analysis found the crude incidence of Rh hemolytic disease of the newborn fell 65%, from 40.5 per 10,000 total births to 14.3 per 10,000.[5]
- Later routine practice: postpartum prophylaxis reduced alloimmunization in at-risk pregnancies from about 13% to 16% to about 0.5% to 1.8%, and routine antepartum plus postpartum prophylaxis pushed rates lower still, to roughly 0.14% to 0.2%.[4]
1. Before prophylaxis, the disease lived in the sequence between pregnancies
Rh disease was always a timing problem before it was a drug story. MedlinePlus still explains the old pattern in the simplest useful way: firstborn infants are often not affected unless the mother had a prior sensitizing exposure, because it takes time for maternal antibodies to develop; later Rh-positive children are the ones more likely to be hit.[1] That sequence is why the condition felt so cruel in practice. One pregnancy could look ordinary. The next could carry hemolysis, rising bilirubin, hydrops, or fetal loss.
StatPearls makes the immunology behind that sequence even clearer. Maternal alloimmunization can begin when fetal red cells enter the maternal circulation, and the threshold can be very small: as little as 0.1 mL of fetal blood may be enough to sensitize the mother.[2] That fact matters because it explains why delivery, miscarriage, invasive procedures, trauma, and other fetomaternal hemorrhage events became such intense obstetric attention points later on. Once you understand that tiny exposures can matter, prevention stops looking like a vague good practice and starts looking like time-sensitive damage control.
This is also why nursery treatment, however important, could never be the whole answer. Exchange transfusions and phototherapy treat the infant after maternal immunity has already crossed the placenta and started destroying fetal or neonatal red cells.[1] They are downstream medicine. The decisive post-1968 change was upstream: intercept sensitization before the mother's immune memory hardens into the problem carried into the next pregnancy.[2][3]
2. The 1968 breakthrough changed obstetrics by changing the unit of action
The Columbia history of RhoGAM is useful because it preserves how strange the solution first looked. The prophylactic agent was itself anti-Rh antibody, which meant physicians were using the very specificity that caused the disease to prevent sensitization in the first place.[6] That paradox is part of the event. The breakthrough was not obvious common sense. It was a counterintuitive but workable immunologic intervention that converted a repeating maternity tragedy into a preventable exposure event.
FDA's current prescribing information shows how thoroughly that idea has since been operationalized. The insert records 1968 as the drug's initial U.S. approval and gives the modern sequence in a form that reads less like drama than protocol: antepartum prophylaxis at 26 to 28 weeks gestation, administration within 72 hours of suspected or proven exposure to Rh-positive red cells after sensitizing events, and postpartum administration within 72 hours of delivery if the newborn is Rh-positive.[3] That is the historical transformation in one block of regulatory prose. The disease became legible as a checklist.
Inference from the regulatory language and the historical accounts: RhoGAM did not merely add one more injectable product to maternity care. It changed what good prenatal care had to include. A pregnancy could no longer be managed on clinical impression alone. It required blood typing, antibody surveillance, documentation of sensitizing events, and an explicit handoff from delivery room to postpartum prophylaxis.[1][3][6]
3. The key move was to turn birth into a clock, not just an outcome
The most important line in the FDA insert may be the plainest one: postpartum RhoGAM should be administered within 72 hours of delivery when the newborn is Rh-positive.[3] That sentence explains why Rh disease became a logistics test. Once the clinical team knows maternal Rh status and infant Rh status, the relevant question is no longer theoretical risk alone. It is whether the system can execute on time.
MedlinePlus shows how that execution entered routine patient-facing care. Rh-negative mothers are followed closely during pregnancy, receive RhoGAM during the second trimester, and receive another dose within a few days after delivery if the baby is Rh-positive.[1] The elegance of the preventive model is that it works by disciplining ordinary moments in obstetric care rather than waiting for catastrophic signs in the infant. A blood type, a lab result, a postpartum order, a signed administration record: these became the real anti-Rh architecture.
The dose logic also reveals that prophylaxis was never treated as decorative. FDA's current label says additional postpartum doses are indicated when maternal exposure exceeds 15 mL of Rh-positive red blood cells.[3] That is another clue to what changed historically. Prevention was not a symbolic shot of reassurance. It was built as quantified exposure management.
4. The public-health effect was large because the workflow held
The epidemiology after approval shows why this mattered. A 1982 U.S. incidence study reported that Rh hemolytic disease of the newborn dropped 65% during the 1970s, from 40.5 per 10,000 births in 1970 to 14.3 per 10,000 in 1979.[5] A more recent prevalence review traced the same arc in longer form, describing RhD prophylaxis as the intervention that moved at-risk alloimmunization from roughly 13% to 16% down to 0.5% to 1.8% with postpartum administration and lower still once routine antepartum prophylaxis was added.[4]
Those numbers matter because they show what kind of invention RhoGAM really was. Some medical breakthroughs work because a new machine or molecule rescues the sickest patients one by one. This one worked because it inserted a reliable step into the ordinary pathway of care. The reduction was population-scale precisely because the intervention could be attached to routine prenatal visits, delivery records, and postpartum dosing windows.[3][4][5]
That is also why the Columbia anniversary account emphasizes both the speed and the administrative struggle behind launch. The release date was pushed forward, and the first patient received RhoGAM on May 29 at Holy Name Hospital in New Jersey.[6] The story is not only laboratory discovery. It is accelerated translation into standard care.
5. Why Rh disease did not disappear completely
It would be easy to turn this into a solved-history piece. The modern sources resist that simplification. StatPearls notes that despite standardization, about 0.1% to 0.4% of at-risk women still become sensitized during pregnancy, often because of antigens other than RhD.[2] The condition has become rarer in settings with good prenatal care, not biologically impossible.[1][2]
That residual burden matters for two reasons. First, it keeps the historical lesson honest: prophylaxis succeeded because systems got better, and systems can still miss. A patient may present late, a sensitizing event may go unrecognized, a large fetomaternal hemorrhage may require dose escalation, or the antibody problem may involve something other than RhD.[2][3] Second, it shows the limit of nostalgic medical storytelling. The great breakthrough did not abolish fetal-maternal blood incompatibility. It made one major branch of it governable.
Why this reconstruction still matters
The strongest way to remember Rh disease in 2026 is not as an old nursery pathology or a triumphalist drug anecdote. It is as one of the clearest examples of modern medicine turning a catastrophic pattern into a timed prevention protocol.[1][3][5] Blood typing identified risk. Serology tracked sensitization. RhoGAM gave obstetrics an intervention that had to be delivered at the right gestational moments and again after birth if the infant was Rh-positive.[1][3]
That sequence changed the emotional shape of care. Before prophylaxis, families often discovered the problem only after a baby was already ill. After prophylaxis, the center of action moved earlier, into paperwork, screening, and the postpartum clock. The rescue image receded; the protocol remained. That is why this history still feels modern. It is not only about a drug. It is about what happens when prevention becomes an ordinary part of the care path instead of a heroic afterthought.
Sources
- MedlinePlus Medical Encyclopedia, "Rh incompatibility" - current clinical overview covering why first pregnancies are often spared, how later pregnancies are put at risk, and how second-trimester plus postpartum RhoGAM changed routine prevention.
- StatPearls / NCBI Bookshelf, "Hemolytic Disease of the Fetus and Newborn" - mechanism review noting that as little as 0.1 mL of fetal blood can sensitize the mother, that Rh prophylaxis entered practice in 1968, and that Rh-induced HDFN prevalence has fallen substantially since then.
- U.S. Food and Drug Administration, RhoGAM and MICRhoGAM Package Insert - current prescribing information listing initial U.S. approval in 1968, prophylaxis at 26 to 28 weeks, postpartum administration within 72 hours, and additional dosing after larger fetomaternal hemorrhage.
- Bennett RL et al., "Live birth prevalence of hemolytic disease of the fetus and newborn in the United States from 1996 to 2010" (Journal of Blood Medicine, 2023; PMC) - prevalence review summarizing the large fall in RhD alloimmunization after postpartum and antepartum prophylaxis.
- Cummins RO et al., "Rh hemolytic disease of the newborn: using incidence observations to evaluate the use of RH immune globulin" (American Journal of Public Health, 1982; PMC) - U.S. incidence analysis showing a 65% drop during the 1970s.
- Columbia University Irving Medical Center, "RhoGAM at 50: A Columbia Drug Still Saving Lives of Newborns" - institutional history of the drug's development and first clinical use in May 1968.
- Wikimedia Commons, "File:Blood Types.jpg" - source page for the documentary clinical blood-typing photograph used as the article image.