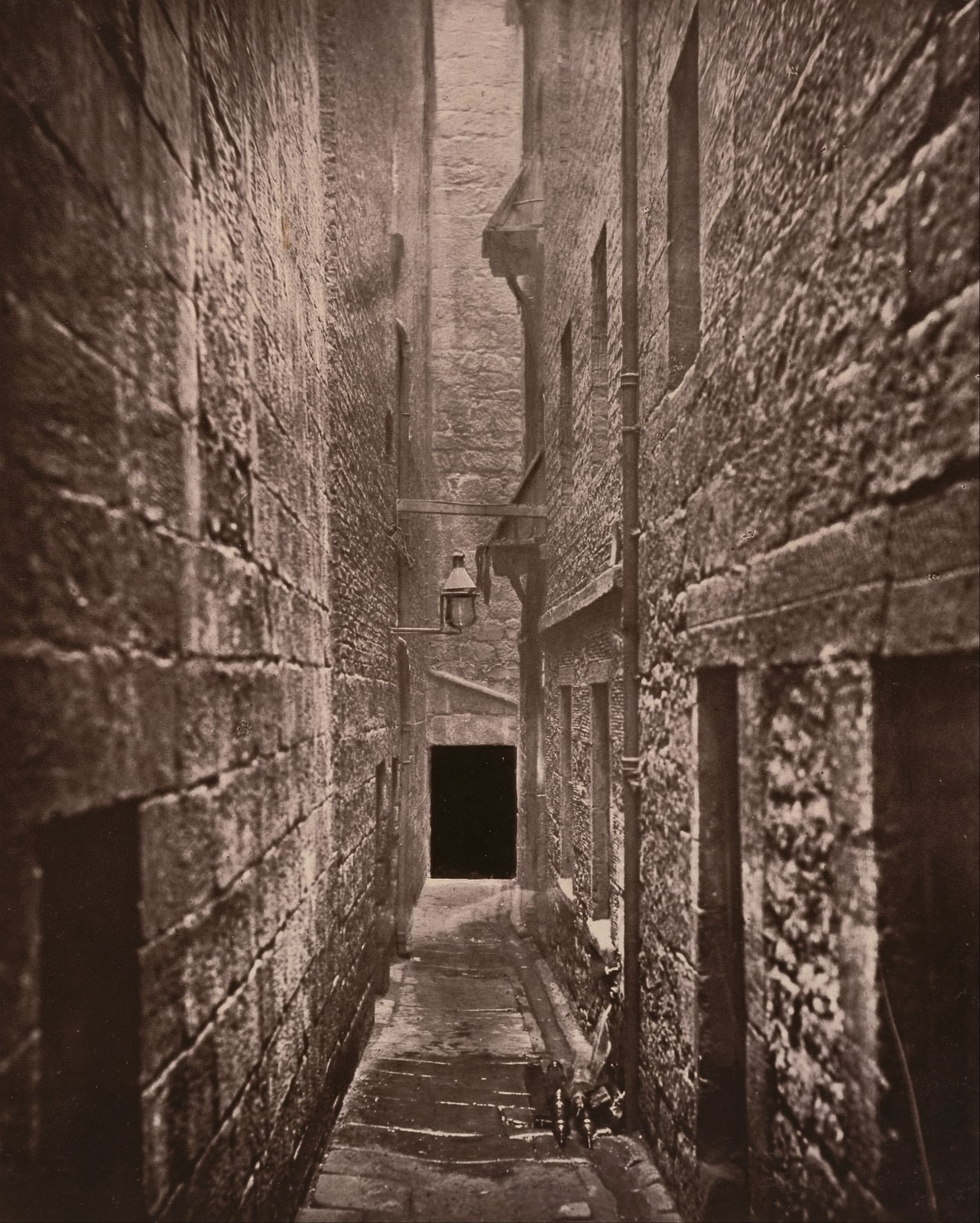
The photograph is an argument in stone. Between 1868 and 1877, Thomas Annan aimed his camera into Close No. 61 off Glasgow's Saltmarket: high walls, a pinched passage, a drainage channel, and little light. It refuses to keep the candidate causes of mortality decline in separate boxes. A higher wage could change what a household ate; municipal works could change its water and waste; housing reform could change its exposure to damp, crowding, and stale air. The mechanisms entered bodies through the same street.[4][5][8]
A century later, the physician and historian Thomas McKeown asked who deserved credit for that transition. His answer was deliberately unsettling. The great fall in death from infectious disease, he argued, began too early for most effective drugs and had too much to do with diseases untouched by sanitary engineering for medicine or public health to claim the victory. Rising living standards—above all, better nutrition—did most of the work.[1][2]
McKeown's intervention was valuable because it broke a flattering story in which doctors steadily rescued modern society. It became misleading when one broken master narrative hardened into another. The best evidence now supports neither “medicine saved us” nor “food saved us.” Mortality fell through different mechanisms at different ages, in different places, on different timelines. McKeown was strongest as a critic of medical triumphalism and weakest as the author of a single replacement cause.[2][4][5]
First, Define What Changed
“People lived longer” compresses several distinct changes. Period life expectancy at birth in England and Wales rose from 40.2 years for males and 42.3 for females in 1841 to 78.6 and 82.6 years in 2020, according to the Office for National Statistics. Yet the most common age at death among people aged ten and over was already 75.6 in 1841. The roughly 35-year gap between that mode and life expectancy at birth was driven largely by deaths in infancy and childhood.[7]
That distinction changes the causal question. An intervention that keeps infants from dying of diarrhoea can transform life expectancy at birth without moving the typical age at which an older adult dies. A factor that reduces adult tuberculosis may operate earlier than the municipal system that cuts childhood enteric disease. A treatment introduced in the 1940s cannot explain a decline observed in the 1840s, but it may matter greatly to the later part of the same disease curve.
The argument therefore needs at least three clocks. The first is the long decline in crisis mortality and adult infection beginning before the Victorian sanitary state. The second is the sharp late-19th- and early-20th-century improvement in infant and child survival. The third is the mid-20th-century expansion of effective vaccination, antimicrobial treatment, safer obstetrics, and chronic care. Treating those clocks as one event all but guarantees a false winner.[2][5][7]
McKeown's Case: The Treatments Arrived Late
From 1955 through 1972, McKeown developed his explanation in a series of demographic papers; in 1976, he carried it into two influential books. His method was to work backward from cause-of-death trends. If mortality from a disease was already falling before a specific therapy or preventive measure became available, that measure could not have started the decline.[2]
Tuberculosis gave the argument its force. In McKeown and R. G. Record's analysis of England and Wales, tuberculosis accounted for 47.2 percent of the reduction in mortality between 1851–60 and 1891–1900. The combined category of typhus, enteric fever, and continued fever accounted for 22.9 percent, while scarlet fever accounted for 20.3 percent.[1] Tuberculosis had no curative drug during that period, and it was not primarily a waterborne infection. If it supplied the largest share of the fall, neither antibiotics nor sewers could be the universal explanation.
McKeown rejected declining pathogen virulence as an adequate general answer and reasoned that better-fed bodies were more able to survive infection. The wider increase in food supply and material living standards, rather than a sequence of heroic clinical discoveries, became his main mechanism.[1][2]
One part of that case remains hard to dismiss: much of the 19th-century mortality decline preceded effective curative medicine. Streptomycin did not reach tuberculosis patients until the 1940s; the mortality curve had been moving for decades. Any account that simply projects the power of later medicine backward is chronologically impossible.[2][4]
The Nutrition Interpretation: Right Scale, Weak Isolation
The strongest defense of McKeown does not claim that calories explain everything. It argues that he chose the right scale. Income, food, housing, workload, and exposure shape whether infection becomes fatal long before a patient reaches a clinic. Bernard Harris's 2004 reassessment gives nutrition a place within a “battery” of interacting causes rather than restoring it as a sovereign one. Aleck Ostry and John Frank similarly argue that nutrition and changing environments remain plausible drivers of the earlier decline in adult mortality, especially tuberculosis, while the later fall in infant and early-childhood mortality followed a different pattern.[4][9]
This interpretation fits an important biological truth: infection and nutritional status can reinforce each other. Poor nutrition may weaken resistance and recovery; repeated infection can suppress appetite, impair absorption, and deepen nutritional loss. Better wages may buy more food, less crowded housing, cleaner fuel, or time away from dangerous work. “Living standards” names a bundle, not an isolated treatment.
That is also the weakness in using nutrition as the residual explanation. Once late medicine, declining virulence, and a narrow definition of sanitation have been ruled out, the remainder does not automatically become food. National food availability is not individual nutritional status. Average wages do not show how food was distributed within households. Tuberculosis mortality may respond to crowding, workplace exposure, isolation practices, milk safety, and changing diagnostic labels as well as diet.[2][3][4]
McKeown successfully demonstrated that a treatment introduced after a decline cannot have initiated it. He did not, by chronology alone, demonstrate which earlier exposure did.
The Intervention Interpretation: Public Health Was More Than Pipes
Simon Szreter's challenge—issued as a discussion paper in 1986 and published in journal form in 1988—attacked both the disease arithmetic and the category boundaries. McKeown's separation of tuberculosis from bronchitis and pneumonia leaned on historical death certificates whose labels were unstable. More fundamentally, “public health” had been defined too narrowly if it meant only a few technologies aimed at obviously waterborne diseases. Local administration, housing regulation, sanitary inspection, safer milk, waste removal, maternal and infant services, and the political capacity to enforce standards were also interventions.[2][3]
The point is not that every sanitary reform worked as advertised. Early public-health policy was shaped by miasma theory, uneven enforcement, local resistance, and imperfect engineering. The point is that a rising standard of living was not merely an invisible market tide. Clean water required reservoirs, pipes, loans, taxes, land, engineers, and maintenance. Less contaminated food required inspection and regulation. A safer street or tenement was partly income and partly government.
The chronology in Britain supports a substantial, but bounded, intervention case. The Public Health Acts of 1848, 1872, and 1875, together with the Sanitary Act of 1866, expanded the framework for local action. Recent research on English cities does not find one instant sanitary revolution. It finds sequencing: early water investments were associated with substantial reductions in infant and childhood mortality in a small four-town sample from 1845 to the mid-1880s, while later sewerage capital worked in tandem with water infrastructure.[5]
That age pattern matters. The study did not find an adult-mortality effect from the early water investments. It therefore does not refute every part of McKeown's adult-tuberculosis story. It does refute the habit of treating an aggregate national decline as if every age group traveled by the same route.[5]
Newer Studies Replace Attribution With Identification
The original debate often compared timelines: did a disease fall before or after an intervention? Newer studies try to exploit variation in when cities adopted infrastructure, how much they invested, or what constrained them. That does not remove uncertainty, but it asks a stronger causal question than simple coincidence.
David Cutler and Grant Miller's original study of major U.S. cities in the early 20th century estimated that filtration and chlorination accounted for nearly half of the reduction in total mortality, three-quarters of the infant-mortality decline, and nearly two-thirds of the child-mortality decline in their sample.[6] Those figures are neither portable estimates for Victorian Britain nor the last word on the U.S. data. A reanalysis of 25 cities from 1900 to 1940 estimated that filtration reduced infant mortality by 11–12 percent but found no measurable mortality effect for the other interventions it studied.[10] Cutler and Miller's reply, after correcting acknowledged data errors, still attributed 38 percent of the total-mortality decline to filtration.[11] The disagreement turns on data construction and model choices; together, the studies make sanitation powerful but contested comparative evidence, not a universal coefficient.
The 2023 English-city study by Toke Aidt, Romola Davenport, and Felix Gray is more directly relevant and more modest. Across 16 large provincial urban districts from 1880 to 1909, the authors estimate that sewerage capital could explain about 13 percent of the decline in all-cause mortality. Water capital's direct effect was imprecise in most specifications, but water appeared to strengthen the effect of sewerage. The authors also stress the limits: only four towns had the longer early-water series, investment and mortality geographies do not align perfectly, and the pathway from sewerage to the measured causes of death remains uncertain.[5]
That combination—an effect, a mechanism hypothesis, and a visible uncertainty boundary—is more useful than a totalizing verdict. It says infrastructure mattered, sometimes greatly, without making every mortality decline a sewer story.
Why The Causes Refuse To Stay In Separate Boxes
The debate's deepest problem is that its candidate causes interact. Nutrition is safer when food is not repeatedly contaminated. A piped water supply works better when sewerage removes fecal waste instead of moving it into the next household's source. Higher wages can improve diet; the same tax base can finance a reservoir. Lower crowding can reduce tuberculosis transmission; better nutrition can improve the outcome after exposure. Later, vaccination and treatment act on a population whose risks have already been reshaped by those environmental changes.[4][5]
The unit of analysis also changes the answer. For adult tuberculosis before 1900, material conditions and exposure may dominate. For urban children facing enteric disease around 1900, water, sewerage, milk safety, and household hygiene become more prominent. For bacterial infection after the 1940s, antimicrobial treatment can sharply alter case fatality even when it did not begin the earlier decline. “What caused mortality to fall?” is too broad until it specifies disease, age, place, and interval.
Better evidence could still move the balance. The nutrition case would strengthen with individual-level records linking diet or nutritional status to cause-specific survival before sanitary change. The intervention case would strengthen with more towns, better-matched administrative boundaries, and credible shocks to the timing of water, sewerage, housing, or food-safety programs. Both would improve with death records reclassified under consistent diagnostic rules. What would not settle the argument is another national curve with one favored invention drawn on top.
What Survives The Debate
McKeown's durable achievement was to make timing an ethical check on professional memory. Medicine should not claim deaths it did not yet know how to prevent. His error was to treat what remained after that correction as evidence for a dominant nutritional cause.[2][4]
Szreter and later public-health historians restored agency, but the strongest version of their case is not another victory parade. Sanitary systems were gradual, politically contested, technically complementary, and uneven in whom they protected. Modern causal studies show sizable effects in particular settings while also showing why those estimates cannot be universalized.[3][5][6]
The mortality decline was less like one discovery than a relay. Food, wages, housing, water, sewerage, regulation, behavior, vaccination, and treatment took the baton at different points; sometimes two had to move together before either registered in the death rate. The brick tunnels in the photograph are not the whole answer. They are a reminder that survival can be built collectively—and that the work may disappear beneath the city once it succeeds.
Sources
- Thomas McKeown and R. G. Record, “Reasons for the Decline of Mortality in England and Wales During the Nineteenth Century,” Population Studies 16, no. 2 (1962) — original cause-of-death decomposition and chronology.
- James Colgrove, “The McKeown Thesis: A Historical Controversy and Its Enduring Influence,” American Journal of Public Health 92, no. 5 (2002) — full historical reconstruction of the thesis, criticism, policy context, and surviving questions.
- Simon Szreter, “The Importance of Social Intervention in Britain's Mortality Decline c.1850–1914: A Reinterpretation,” CEPR Discussion Paper 121 (1986; published in journal form in 1988) — foundational intervention-centered critique.
- Bernard Harris, “Public Health, Nutrition and the Decline of Mortality: The McKeown Thesis Revisited,” Social History of Medicine 17, no. 3 (2004) — qualified defense of nutrition as one interacting cause.
- Toke S. Aidt, Romola J. Davenport, and Felix Gray, “New Perspectives on the Contribution of Sanitary Investments to Mortality Decline in English Cities, 1845–1909,” Economic History Review 76 (2023) — city-level estimates, timing, complementarity, and limitations.
- David M. Cutler and Grant Miller, “The Role of Public Health Improvements in Health Advances: The Twentieth-Century United States,” NBER Working Paper 10511 (2004; published in Demography, 2005) — causal estimates for filtration and chlorination.
- Office for National Statistics, “Mortality in England and Wales: Past and Projected Trends in Average Lifespan” (2021) — historical life expectancy, modal age at death, and infant-mortality context.
- Wikimedia Commons, “Thomas Annan, Close, No. 61 Saltmarket” — public-domain carbon print photographed in Glasgow between 1868 and 1877, from the J. Paul Getty Museum, used as the article image.
- Aleck S. Ostry and John Frank, “Was Thomas McKeown Right for the Wrong Reasons?” Critical Public Health 20, no. 2 (2010) — age-specific reassessment of adult and early-life mortality mechanisms.
- D. Mark Anderson, Kerwin Kofi Charles, and Daniel I. Rees, “Reexamining the Contribution of Public Health Efforts to the Decline in Urban Mortality,” American Economic Journal: Applied Economics 14, no. 2 (2022) — expanded-data reanalysis of U.S. water interventions and infant mortality.
- David M. Cutler and Grant Miller, “Comment on ‘Reexamining the Contribution of Public Health Efforts to the Decline in Urban Mortality,’” American Economic Journal: Applied Economics 14, no. 2 (2022) — corrected-data reply and alternative estimate.