Three Mile Island is often remembered as the American nuclear accident: the one that frightened the country, scarred the industry's reputation, and became shorthand for "meltdown."[1][4] That memory is not wrong, but it can flatten the event into a single image of reactor danger. The sharper historical question is narrower and more revealing: how did a problem that began with the loss of feedwater on the plant's secondary side become, within hours, a partial core-melt accident inside Unit 2? The answer is not one dramatic explosion or one villainous decision. It is a sequence in which hardware failure, control-room interpretation, and emergency procedure drifted out of alignment.[1][2][3]
On March 28, 1979, the plant did have mechanical failures. It also had automatic safety systems that initially did what they were supposed to do.[1][2] What made the morning dangerous was that the most important signals were not the ones the operators thought they were reading. A relief valve opened and did not re-close, yet the control board suggested the command to close had been sent.[1] Pressurizer level appeared high, even while steam voids were forming elsewhere in the reactor coolant system.[2] Emergency core cooling started, but operators reduced it because the instrumentation picture they trusted implied that the reactor held too much water, not too little.[2][3] Three Mile Island became historic because the plant's panel logic, human assumptions, and procedural habits no longer described the same physical reality.
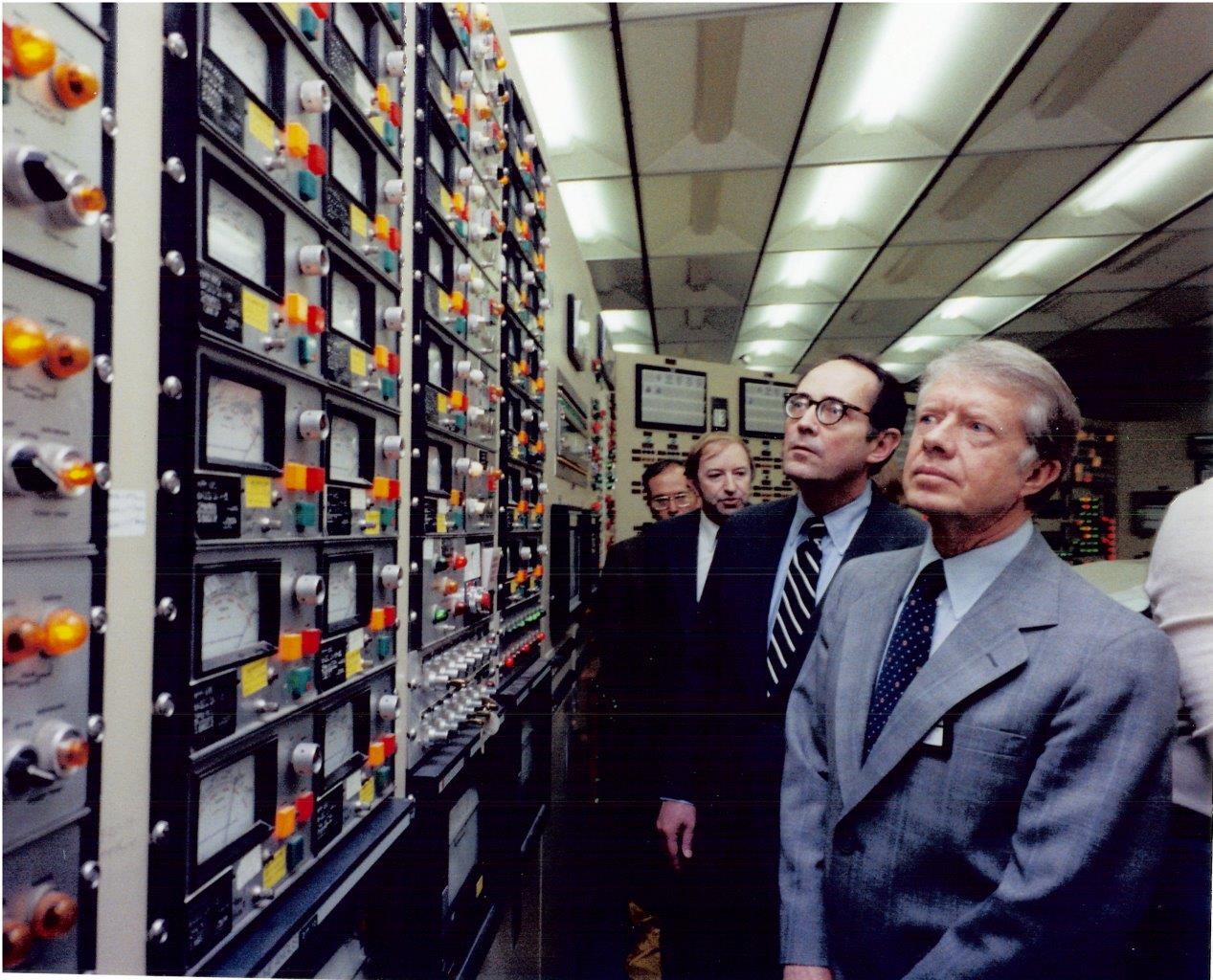
The control-room image used here was taken on April 1, 1979, when President Jimmy Carter toured TMI-2 with Governor Dick Thornburgh and NRC official Harold Denton.[6][7] It is the right image for this reconstruction because it does not show the damaged core. It shows the room in which the accident had to be interpreted. By the time Carter arrived, the story had already expanded from a plant transient into a national crisis of reassurance, explanation, and credibility.[5][6]
1) The first eight minutes: a routine transient loses its shape
The initiating event was not exotic. At about 4:00 a.m. on March 28, the secondary system lost feedwater.[1][2] That, in turn, tripped the turbine and then the reactor, which is the kind of protective sequence designers expect a pressurized-water reactor to survive.[1] The problem was that the chain did not stop there. The pressurizer's pilot-operated relief valve opened during the initial pressure surge, as designed, but then failed to close when the pressure dropped below its actuation point.[1][2] Coolant continued to escape through a path the operators did not yet understand to be open.
At almost the same time, the plant lost one of the most basic recovery tools it should have had available. NRC's April 5 preliminary chronology states that by t = 30 seconds all three auxiliary feedwater pumps were running, but no flow entered because the discharge valves were closed.[2] The same bulletin states that auxiliary feedwater flow did not actually begin until t = 8 minutes, after those closed valves were opened.[2] That eight-minute gap matters because it turns a manageable transient into a drying-out steam-generator problem. The plant had backup water on paper; in the event, it did not have it at the point that counted.
This is the first reason Three Mile Island should be reconstructed as a sequence rather than a symbol. The accident did not begin with a bare technological incapacity. It began with the dangerous coexistence of available safety systems and unavailable safety function. The pumps could run. The water still did not arrive. That distinction is the kind operators only get credit for noticing if their procedures, indications, and recovery checks are built for it.[2][3]
2) The stuck valve mattered because the board did not display the right fact
The relief valve failure became decisive for the same reason. What the operators saw on the panel was not a direct indication that the valve itself remained physically open. They saw that the signal to close it had been sent.[1] That difference between command status and actual valve position has become one of the canonical lessons of the event, because it meant the room was organized around a reassuring but incomplete fact.[1][3][4]
Meanwhile, coolant was leaving the reactor coolant system. NRC's bulletin describes the consequence in blunt terms: the pressurizer level indication may have led to erroneous inferences of high water inventory in the reactor coolant system, even though substantial voids existed elsewhere.[2] This is the second key turn in the reconstruction. Operators were not irrationally ignoring danger. They were trying to control the plant through an instrument hierarchy that made one part of the system look full while another part was moving toward uncovering and heat-up.[2][3]
That is why the Three Mile Island story cannot be reduced to "human error" in the easy moralizing sense. The humans in the room did make consequential mistakes. But the historical mechanism sits in the coupling between the mistaken action and the misleading architecture of information. If a display tells you the relief path is closed and the pressurizer looks overfilled, then reducing emergency injection can feel like preserving control rather than abandoning it.[1][2]
3) From protection to damage: why the operators backed away from cooling
The chronology of the first two hours is brutal because it shows protective systems being turned into liabilities by misread conditions. NRC's bulletin records that emergency core cooling began at t = 2 minutes when pressure dropped to the setpoint for high-pressure injection.[2] But the same chronology records that one HPI pump was manually tripped at about 4 minutes 30 seconds, and the second at about 10 minutes 30 seconds.[2] In other words, automatic safety injection started correctly and was then reduced by operators who believed they were preventing the system from becoming overfilled.[2][3]
This is where the relief valve, the pressurizer indication, and operator judgment all lock together. If the operators had correctly understood that coolant was still escaping, emergency injection would read as compensation. Because they did not, injection could instead look like overcorrection. The room's picture of the reactor had split from the reactor's actual state.[1][2][3]
The later chronology shows how expensive that misunderstanding became. At about 1 hour 15 minutes, operators tripped the reactor coolant pumps in one loop; at about 1 hour 40 minutes, they tripped the pumps in the other loop, partly out of concern for pump damage from vibration.[2] NRC's bulletin later identified this as one of the six critical failure points, noting that pump trips during the transient contributed to fuel damage because large voids prevented natural circulation from carrying heat away effectively.[2] By roughly 1.75 to 2 hours, the core had entered a heat-up transient, and at about 2.3 hours the relief valve was finally isolated by operator action.[2] The plant had, by then, spent far too long losing coolant through a path that the control room had not treated as the central emergency.
Seen in sequence, the accident looks less like one instant of collapse than like a repeated tendency to act on the wrong abstraction. The operators were managing level, pressure, and pump behavior. What the core needed was sustained cooling and a better grasp of inventory loss. The gap between those two realities is the heart of the event.[2][3][4]
4) The plant accident became a public crisis when hidden paths turned into visible confusion
Three Mile Island did not remain only a control-room story. NRC's April 5 bulletin says that because containment did not isolate on high-pressure injection initiation, highly radioactive water from the relief-valve discharge was pumped out of containment by automatic transfer, entered the auxiliary building's waste-treatment system, and overflowed there; outgassing from this water through the auxiliary-building ventilation system became the principal source of offsite noble-gas release.[2] That point matters historically because it joins the technical and public sides of the event. A plant already being misread inside the control room was now producing effects that had to be explained outside it.
The national drama that followed was not simply a matter of radiation dose. NRC's later summaries stress that the accident produced no detectable health effects among the nearby population.[1] But health outcome and public confidence are not the same category. The event became a civic emergency because conflicting statements, uncertain recommendations, and partial technical understanding reached the public in real time.[4][5][6] Carter's April 11, 1979 executive order creating the President's Commission on the Accident at Three Mile Island is revealing on this point: the commission was directed not only to assess technical causes and NRC oversight, but also to evaluate how the public's right to information had been served and what should change to provide accurate, comprehensible, timely information during similar emergencies.[5]
That clause is easy to overlook, but it is one of the clearest windows into what Three Mile Island did to American governance. The accident was not judged to be only a hardware or operator problem. It was also understood as a failure in public explanation. Carter made the same point more directly after visiting the site on April 1, promising to be personally responsible for thoroughly informing the American people and making the investigation public.[6] The control-room photograph therefore captures more than a presidential inspection. It marks the moment when a technical transient became a national test of trust.
5) Why the event still matters
The long afterlife of Three Mile Island sits in the reforms that followed: operator training changes, stronger emergency preparedness, more attention to human factors and control-room design, tighter operating discipline, and a broader recognition that severe accidents cannot be understood only as equipment failures.[1][3][4] In retrospective summaries, the NRC also points to institutional changes in emergency response and oversight, while later industry and laboratory accounts emphasize communication as a core element of emergency planning.[1][4]
But the historical force of the event is present before the reforms. It sits in the pattern of the first morning. A secondary-side disturbance triggered a protective shutdown. A relief valve stuck open. Auxiliary feedwater existed but did not initially flow. An instrument picture suggested the wrong problem. Emergency injection was reduced. Pumps were stopped. Heat built in the core. Radioactive water took an indirect route into the auxiliary building, and the struggle to explain what had happened began almost before the plant itself was stable.[1][2][3]
That is why Three Mile Island remains worth reconstructing in detail. It was not simply the day Americans discovered that reactors could fail. It was the day a modern control system demonstrated how dangerous partial knowledge can be when a room full of professionals acts on indicators that are true in one narrow sense and false in the one that matters most. The accident's lasting lesson is not panic. It is mismatch: between command and condition, between instrumentation and physical state, and between technical uncertainty and the public demand to know what is happening now.[1][2][5][6]
Sources
- U.S. Nuclear Regulatory Commission, "Backgrounder on the Three Mile Island Accident."
- U.S. Nuclear Regulatory Commission, "Bulletin 79-05A: Nuclear Incident at Three Mile Island - Supplement" (April 5, 1979).
- U.S. Nuclear Regulatory Commission, TMI-2 Lessons Learned Task Force Final Report (NUREG-0585).
- U.S. Nuclear Regulatory Commission, Knowledge Management Digest - Overview (NUREG/KM-0001, Rev. 1).
- Jimmy Carter, "Executive Order 12130-President's Commission on the Accident at Three Mile Island" (April 11, 1979), The American Presidency Project.
- Jimmy Carter, "Middletown, Pennsylvania Remarks to Reporters Following a Visit to the Three Mile Island Nuclear Facility" (April 1, 1979), The American Presidency Project.
- Wikimedia Commons, "File: President Carter in the TMI-2 Control Room.jpg" - image description page citing NRC source, April 1, 1979.