Chronic dialysis is easy to misremember because the machine entered medicine before the treatment really did. By the mid-1940s Willem Kolff had shown that an artificial kidney could clear toxins from the blood and rescue some patients with acute renal failure.[2][6] That was a genuine medical revolution, but it still left one fatal boundary intact. Every treatment required fresh access to arteries and veins, and repeated cannulation damaged those vessels so badly that long-term use for permanent kidney failure remained out of reach.[2][6] The machine worked. The therapy did not yet last.
That is why the decisive event belongs not to the first dialyzer alone, but to the Scribner shunt in Seattle. In March 1960, Belding Scribner, David Dillard, and Wayne Quinton implanted a U-shaped Teflon shunt into the arm of Clyde Shields, a 39-year-old machinist dying of irreversible kidney disease.[2][3] The point was simple and radical at once: keep a stable pathway between artery and vein open after treatment so dialysis could be repeated without destroying the bloodstream each time.[2][5][6] Once that worked, the central question changed overnight. The problem was no longer only whether dialysis could clean blood. It was whether medicine could decide who would receive a treatment that had suddenly become possible but remained scarce.
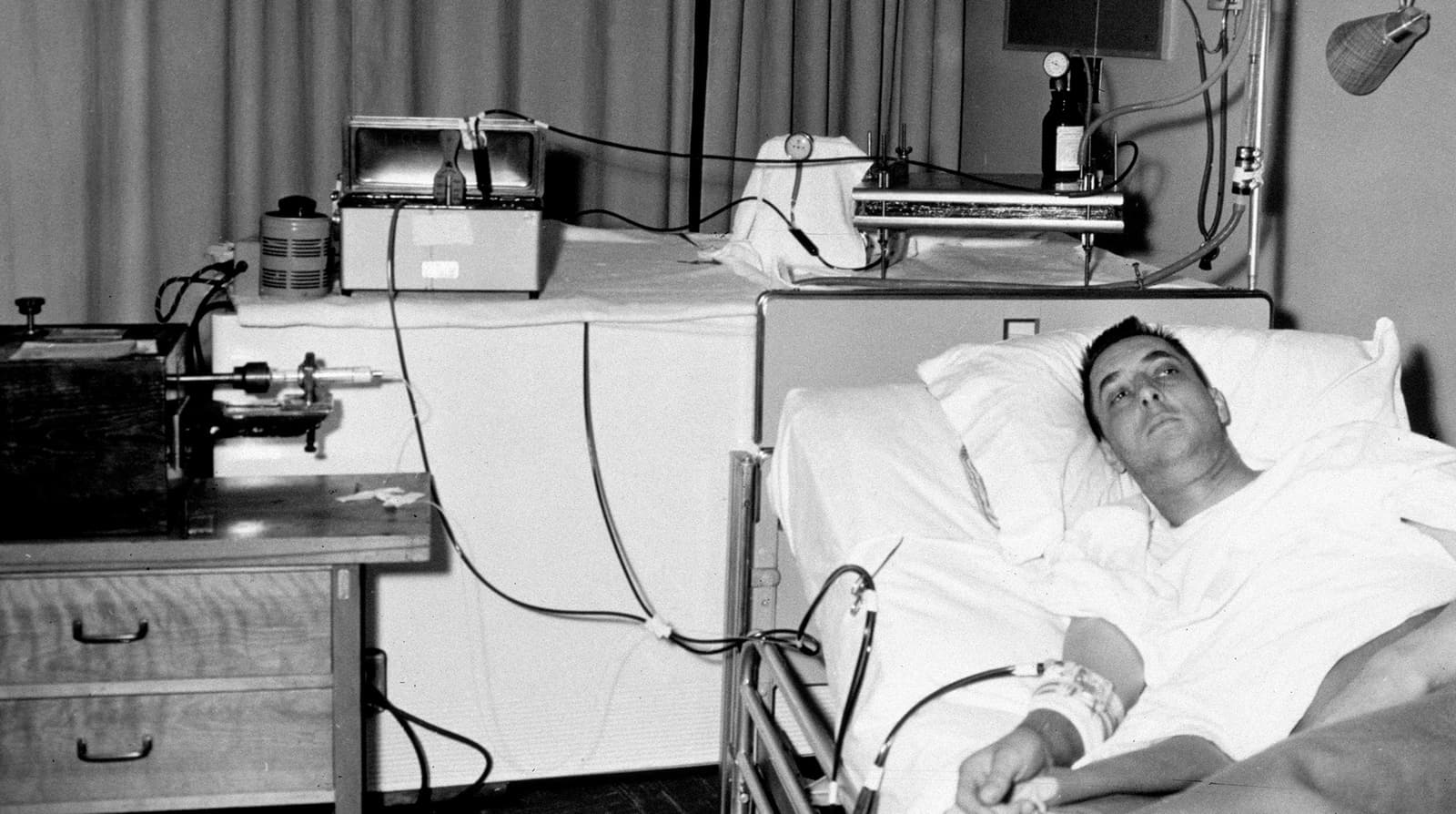
That shift is the real event this article reconstructs. The cover image keeps the story attached to that threshold. It uses an archival University of Washington Magazine photograph of Shields on dialysis because the breakthrough did not arrive as a generic technology trend. It arrived as one patient surviving long enough to prove that repeated access could hold.[3]
Timeline anchors
- 1945: Kolff's rotating-drum artificial kidney achieved its first unequivocal clinical success in acute renal failure, proving blood purification could sustain life for at least some patients.[2]
- March 1960: the first Scribner shunt was implanted into Clyde Shields in Seattle after Wayne Quinton learned how to bend Teflon into a permanent U-shaped arteriovenous bypass.[2][3]
- April 1960: Scribner and colleagues published The technique of continuous hemodialysis, the early formal record of the new treatment pathway.[1]
- 1961: community funding was assembled in Seattle for an outpatient dialysis center because the new treatment could no longer be contained inside occasional hospital rescue.[4]
- 1962-01-09: the Seattle Artificial Kidney Center opened with 3 beds, enough for up to 9 patients receiving overnight dialysis twice each week.[4]
- 1960s: dialysis remained scarce enough that Seattle relied on a lay "Life or Death Committee" to determine who would receive treatment.[4][5]
Those markers show why 1960-1962 is the right frame. The story is not only about a piece of tubing. It is about the short period in which chronic kidney failure moved from technical impossibility into an ethically unstable but real treatment system.
1. Before 1960, dialysis could rescue a crisis but could not become a life
Kolff's machine had already solved one enormous part of the kidney-failure puzzle.[2] Hemodialysis could remove toxic metabolites and buy time during acute, potentially reversible renal injury. Yet for end-stage renal disease, the same success exposed a harder obstacle. The patient's kidneys were not coming back, which meant treatment would have to be repeated over months or years rather than once or twice during a short emergency.[2][6]
That is where access became the bottleneck. The Lasker Foundation's history describes the pre-Scribner situation bluntly: surgeons inserted needles or tubes to access arteries and veins, and after a limited number of sessions those vessels were battered beyond reuse.[2] The recent vascular-access review states the same mechanism more generally. Reliable, repeatable vascular access for outpatient hemodialysis did not exist until the 1960s, when the Quinton-Scribner shunt finally allowed multiple treatments through the same access point.[6]
This boundary matters because it keeps the event from collapsing into a generic "machine got better" story. The central failure before 1960 was not that doctors lacked an artificial kidney capable of moving solutes across a membrane. The central failure was that the human body could not be re-entered indefinitely without ruining the route. A patient with permanent kidney failure therefore remained trapped in a contradiction: there was a machine that could help, but no durable path between the patient and the machine.[2][6]
That is why Kolff's breakthrough and Scribner's breakthrough should not be merged into one seamless invention story. Kolff made dialysis clinically real for acute renal failure. Scribner made repeated dialysis physically repeatable for chronic renal failure.[2][6] The second step was less spectacular in appearance, but it is the step that transformed prognosis.
2. Clyde Shields mattered because one case proved the access loop could stay open
The decisive patient in this reconstruction is Clyde Shields. The Lasker Foundation account says that Scribner, Dillard, and Quinton were ready by March 1960, when they implanted the first shunt into Shields.[2] University of Washington Magazine describes him as a machinist and identifies the image used here as the first patient to receive the shunt that let doctors "tap" the bloodstream repeatedly for dialysis.[3]
The device's logic was austere. Scribner imagined a U-shaped bypass with one end placed in an artery and the other in a vein; when the patient was off dialysis, the system could be capped so blood continued to flow through the shunt itself, preserving access until the next session.[2] When treatment time arrived, staff could connect the artificial kidney to that same loop and then disconnect it afterward.[2][5][6] The new object was therefore not just an accessory to the machine. It was the piece that converted intermittent rescue into maintenance.
What happened next is the best evidence that the threshold had been crossed. Lasker reports that Shields lived for 11 years on intermittent hemodialysis after the shunt was implanted.[2] UW Magazine puts the point more simply: for the first time, kidney failure was no longer an automatic death warrant, because Shields and a few others implanted that year survived.[3] This does not mean the early treatment was smooth, easy, or fully solved. It means the disease had been moved into another category. A patient could now be sustained not merely through an acute episode, but across ordinary calendar time.
That is why the article title uses the word queue. The first successful chronic-dialysis patient did not just prove a biomedical principle. He proved that a new class of claimant now existed. Once people with irreversible kidney failure could stay alive on repeated dialysis, the hospital and the community had to decide how many such lives they could maintain at once.
3. The Seattle center turned a technical triumph into a rationing system
The move from one patient to a treatment program happened quickly. Northwest Kidney Centers records that funding for an outpatient center was assembled in 1961, and that on January 9, 1962 the Seattle Artificial Kidney Center opened as the world's first out-of-hospital dialysis treatment center.[4] The original unit had only 3 beds, enough for up to 9 patients receiving overnight dialysis twice a week.[4] The numbers matter because they expose the scale mismatch immediately. A lifesaving therapy now existed, but its carrying capacity was tiny.
At that point, scarcity stopped being abstract. The same Northwest Kidney Centers history explains that its museum still documents the early Admissions Committee that determined who would receive dialysis and who would not.[4] The University of Washington nephrology history names the problem even more starkly: hemodialysis remained a scarce resource through the 1960s, and treatment was available only to people selected by the "Life or Death Committee," a process it says helped lay the foundation for modern bioethics.[5]
This is the hidden hinge in the dialysis story. The Scribner shunt did not simply add a treatment. It generated a social sorting problem large enough to require explicit selection. Before chronic dialysis became possible, end-stage kidney failure usually ended in death because there was no durable therapy to allocate. After 1960, the problem changed form. There was now a treatment worth fighting over, but too few slots, machines, staff hours, and dollars to extend it to everyone at once.[2][4][5]
That is why the Seattle episode still feels severe in 2026. The rationing did not arise because physicians suddenly became colder. It arose because an engineering success reached medicine faster than institutions could build fair abundance around it. In this sense, the shunt solved one impossibility and exposed another.
4. The real threshold was not the machine alone, but the system that had to grow around it
It would be easy to end the story with moral shock at the committee, but that would miss the larger structural lesson. The Seattle program was not designed to glorify scarcity. It was an improvised system trying to catch up with a treatment that had outrun its infrastructure.[4][5] Chronic dialysis required more than an access device. It required beds, overnight staffing, transport routines, follow-up discipline, funding, and eventually other ways to move treatment beyond the first tiny center.
The early history already points in that direction. Northwest Kidney Centers notes that by 1964 the Seattle program had expanded to 10 stations serving 47 patients, and that home hemodialysis was developed partly because center-based treatment alone was too expensive and too limited in capacity.[4] That later expansion sits just beyond this article's main frame, but it clarifies what the 1960-1962 threshold actually opened. The shunt did not finish chronic dialysis. It created the possibility that forced an entire care system to be invented around it.
Seen this way, the event reconstruction becomes sharper. March 1960 was the access breakthrough. January 1962 was the institutional proof that the breakthrough could be organized outside the hospital. The admissions process was the price of getting there before national capacity and public funding had caught up.[4][5]
Why this 1960-1962 sequence still reads sharply
The strongest conclusion is narrower than triumph and stronger than nostalgia. The Scribner shunt mattered because it changed the unit of impossibility. Before it, chronic kidney failure was mostly a terminal diagnosis because repeated dialysis could not be sustained physically. After it, repeated dialysis could be sustained, which meant death no longer arrived from technical incapacity alone. It also arrived from queue position, money, staffing, and institutional limits.[2][4][5][6]
That is the lasting force of the Seattle story. It shows medicine crossing a line where a patient can be kept alive by a machine often enough to create a new politics of selection. Clyde Shields stands at the beginning of that change because his survival proved that chronic dialysis could leave the status of experiment and enter the status of claim.[2][3] The people who came after him inherited both halves of the breakthrough at once: a real treatment and a real shortage.
The Scribner shunt therefore deserves to be remembered less as a clever tube than as the object that turned kidney failure into a survivable condition and immediately into a public question about who would be allowed to survive.
Sources
- B. H. Scribner, J. E. Caner, R. Buri, and W. Quinton, "The technique of continous hemodialysis" (Transactions - American Society for Artificial Internal Organs, April 1960) - PubMed record for the early formal publication of the new dialysis technique.
- Lasker Foundation, "Hemodialysis for treating end-stage kidney disease" (2002 Albert Lasker Clinical Medical Research Award) - history of Kolff's dialyzer, Scribner's U-shaped shunt, the March 1960 implantation in Clyde Shields, his 11 years on dialysis, and the emergence of the first bioethics committee.
- University of Washington Magazine, "UW dialysis innovation remains a life-saving loophole" - institutional historical feature used for Clyde Shields's March 1960 shunt implantation, the description of him as a machinist, and the archival photograph used as this article's image.
- Northwest Kidney Centers, "Our History" - historical overview used for 1961 funding, the January 9, 1962 opening of the Seattle Artificial Kidney Center, its 3 beds / 9-patient capacity, and the early admissions-committee scarcity structure.
- University of Washington Division of Nephrology, "History of Innovation" - historical page used for the Teflon Scribner shunt, the first outpatient dialysis facility in January 1962, and the note that the "Life or Death Committee" selected patients during the 1960s scarcity period.
- Michael Allon and colleagues, "Hemodialysis Vascular Access: A Historical Perspective on Access Promotion, Barriers, and Lessons for the Future" (Kidney Medicine, 2024; PMC) - review used for the claim that reliable, repeatable outpatient hemodialysis access began in the 1960s with the Quinton-Scribner shunt and that the shunt allowed multiple sessions through the same access.