Cataract surgery is easy to remember as removal: the cloudy lens comes out and light can pass again. That is only half the mechanism. The harder historical turn was replacement. Once the natural crystalline lens is removed, the eye loses a large part of its focusing power. Modern cataract surgery works because it couples extraction with an intraocular lens, or IOL, that restores optical power from inside the eye rather than leaving the patient dependent on thick external spectacles.[2][3]
That shift sounds obvious now because lens implantation has become routine. It was not obvious in 1949. Sir Harold Ridley's leap was to treat the eye not only as a place from which diseased tissue could be taken, but as a place that could safely hold a manufactured optical device. The resulting mechanism joined three things that had to succeed together: a material the eye could tolerate, an optical substitute strong enough to replace a removed lens, and a surgical workflow that could hold the substitute in a stable position.[1][2]
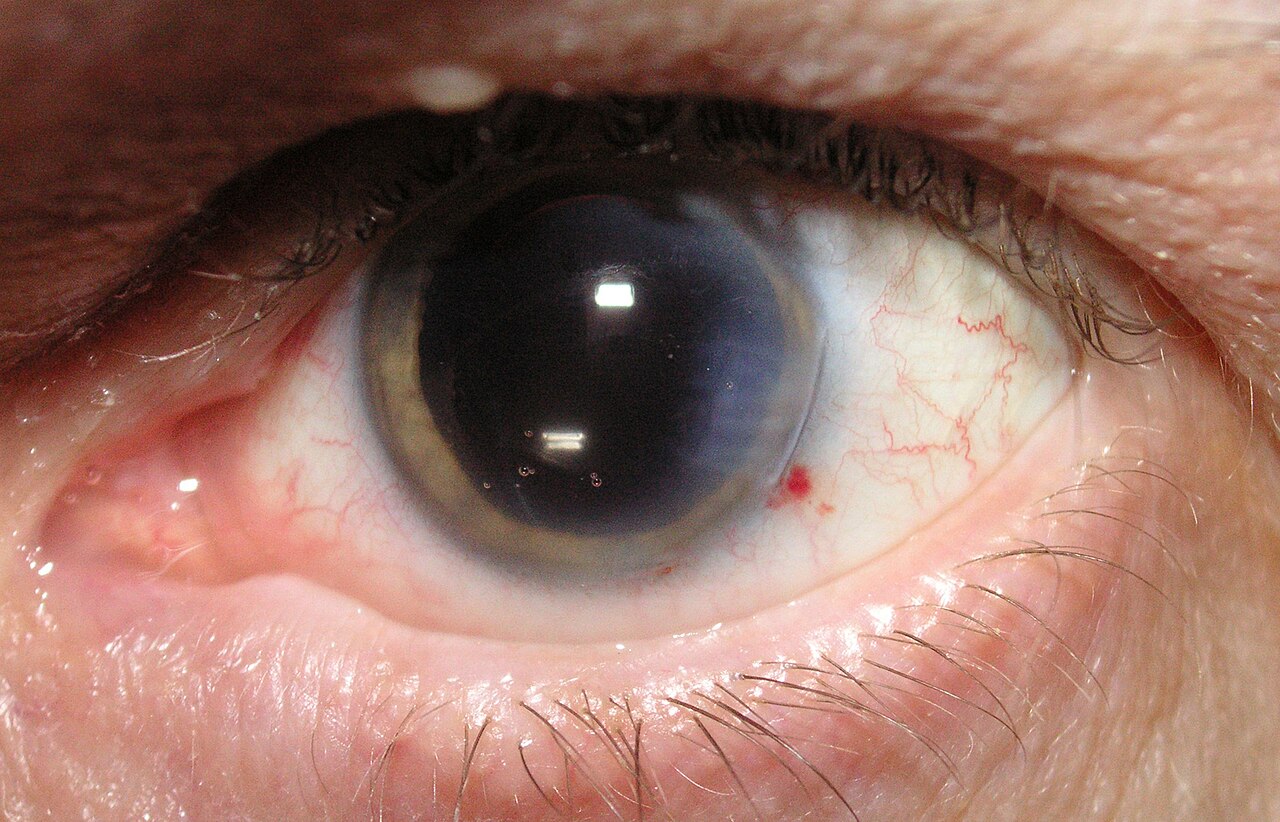
Image context: the cover photograph is a real post-cataract clinical image showing an inserted IOL. It fits because the article is about a physical replacement system, not an abstract improvement in eyesight.[6]
Timeline anchors for the mechanism
- World War II: Ridley observed eye injuries in Royal Air Force casualties and noted that acrylic plastic from aircraft canopies could remain in the eye without the inflammatory rejection associated with glass splinters.[2][4]
- November 29, 1949: Ridley achieved the first IOL implant at St Thomas' Hospital in London; the NCBI Bookshelf history notes that the first permanently retained IOL followed on February 8, 1950.[2]
- 1952: Ridley published "Intra-ocular acrylic lenses after cataract extraction," making acrylic lens implantation a formal surgical proposal rather than only a private experiment.[1]
- Late twentieth century: phacoemulsification and foldable lens materials changed the operation from large-incision removal plus rigid optics toward smaller-incision extraction and capsule-based implantation.[2][4]
- 2024-2026: patient-facing National Eye Institute guidance still describes the core sequence in the same terms: remove the cloudy lens, place the artificial lens, then monitor healing and complications.[3]
1. The missing-lens problem was optical, not cosmetic
The crystalline lens is not just transparent tissue. NCBI's IOL chapter states that it contributes about +15 to +20 diopters of refractive power in the non-accommodative eye, on top of the cornea's focusing contribution.[2] Remove that lens and the patient is no longer simply "clearer." The optical system has been rebuilt with a major element missing.
Before intraocular implantation, that loss had to be compensated from outside the eye with spectacles or contact lenses.[2][5] Thick aphakic spectacles could help central acuity but imposed distortion, magnification, and practical awkwardness. The patient had survived the surgery, but the visual system was still being repaired from a distance. Ridley's question was therefore mechanistic: if the cloudy lens had to come out, could a clear manufactured lens go back into the same optical system?
That is the reason the IOL deserves to be treated as more than a device upgrade. It changed the endpoint of cataract surgery. Removal alone asks whether opacity can be eliminated. Replacement asks whether the eye can be optically reconstructed in place.
2. Acrylic mattered because tolerance had to come before elegance
The first hinge was material. Ridley did not begin with a perfect optical product. He began with a wartime observation: fragments of acrylic aircraft canopy material, later discussed as Perspex or polymethyl methacrylate, could sit in injured eyes without provoking the same reaction as some other foreign bodies.[2][4] That did not prove a lens implant would be safe. It did supply a plausible material clue.
Ridley's 1952 paper placed that clue inside surgery.[1] The early acrylic lenses were rigid, and the operation was controversial for good reasons: implanting a foreign body into the eye carried risks, and early technique had not yet solved all problems of position, inflammation, capsule support, and long-term clarity. The 2026 NCBI overview is useful because it does not romanticize the first generation. PMMA lenses were the first human IOL material, but their rigidity required large incisions and they are now much less used in developed countries.[2]
That history matters because it separates the invention from the polished modern workflow. The causal mechanism was not "plastic is magic." It was a sequence: observe tolerance, shape a clear optical element, implant it where it can do useful refractive work, then keep improving the surgery until the benefit reliably outweighs the risk.
3. The capsule turned replacement into a workflow
Modern cataract surgery depends on anatomy as much as material. The NEI's patient guidance describes the ordinary sequence plainly: the surgeon removes the cloudy lens and places the new artificial lens in the eye.[3] The NCBI surgical overview adds the mechanical detail: a central opening of about 5.5 mm is made in the anterior capsule, the opacified contents are removed, and the IOL is placed within the intact capsular bag when possible.[2]
That capsule support is the quiet engineering achievement. The old lens is not simply swapped like a camera part. The surgeon preserves a holding structure, clears the cloudy contents, and uses the remaining bag as a stable seat for the implant.[2][4] Once that workflow became dependable, the IOL stopped being a heroic insert and became part of a reproducible operation.
Phacoemulsification tightened the mechanism further. NEI describes it as using an ultrasonic probe to break up the hard, cloudy lens tissue through an incision at the front of the eye, then suctioning out the emulsified lens while leaving the capsule in place for the replacement lens.[4] Foldable acrylic and silicone lenses then fit the smaller-incision logic: NCBI notes that flexible lenses can be inserted or injected through incisions generally 3.0 mm wide or less.[2] The lens, the incision, and the capsule became one system.
4. Why the operation became routine without becoming trivial
The scale of modern cataract surgery can hide the fragility of the mechanism. NCBI notes more than 3 million U.S. cataract procedures in 2006 alone, while University of Utah's Moran Eye Center says the United States now sees over 3 million cataract surgeries with IOL implantation each year.[2][5] NEI's patient page says about 9 out of 10 people see better after surgery, while also naming real risks including swelling, bleeding, infection, retinal detachment, pressure changes, and posterior capsule opacity.[3]
That balance is the right way to read the history. The IOL helped make cataract surgery one of medicine's great restoration procedures, but it did not make the eye a risk-free machine. A successful operation still depends on measurement before surgery, lens choice, surgical execution, capsule behavior, healing, and follow-up.[2][3][4] Secondary cataract, or posterior capsule opacification, shows the point especially well: even after the cloudy lens is removed, residual lens cells can later cloud the path behind the artificial lens and require laser treatment.[3][4]
The durable lesson is that cataract surgery became modern when it solved both halves of the problem. Extraction cleared the opacity. The intraocular lens restored the optical missing part. Better incisions, better materials, better capsule placement, and better postoperative management made that replacement repeatable. Ridley's invention mattered because it changed the question from "Can the cloudy lens be removed?" to "Can the eye be rebuilt as a working optical system after removal?"[1][2][4]
Sources
- Harold Ridley, "Intra-ocular acrylic lenses after cataract extraction. 1952" (Bulletin of the World Health Organization, WHO IRIS record for the reprinted 1952 paper).
- John Nguyen and Liliana Werner, "Intraocular Lenses for Cataract Surgery" (Webvision, NCBI Bookshelf PDF, 2026) - optical power, Ridley timeline, PMMA history, capsular-bag workflow, materials, incision size, and U.S. procedure scale.
- National Eye Institute, "Cataract Surgery" (last updated December 5, 2024) - patient-facing summary of removal, IOL placement, recovery, expected vision improvement, and risks.
- National Eye Institute, "NEI charts a clearer future for cataract prevention and treatment" - cataract burden, wartime acrylic observation, phacoemulsification, capsule logic, IOL evolution, and secondary cataract mechanism.
- John A. Moran Eye Center, University of Utah Health, "Intraocular Lens Innovations, Then and Now" (January 22, 2025) - 75-year IOL framing, pre-IOL spectacle burden, current IOL categories, and U.S. annual surgery scale.
- Wikimedia Commons, "File:CataractOperated.jpg" - photographic source page for the clinical image showing cataract surgery performed with an IOL inserted.