The old hookworm myth was cruel because it turned biology into character. In the early twentieth-century American South, fatigue, anemia, slow growth, and poor school performance could be folded into a stereotype about laziness. Rockefeller Archive Center's history of the campaign notes that newspapers helped popularize the "germ of laziness" frame before the Rockefeller Sanitary Commission tried to turn the problem into public-health work.[3] The label stuck because the symptoms looked behavioral from the outside. The evidence points somewhere much more material: human feces in soil, larvae reaching bare skin, worms feeding in the intestine, and communities without the sanitation, shoes, diagnosis, and treatment needed to interrupt the cycle.[1][2]
That distinction matters because hookworm is both intimate and infrastructural. It enters through the skin, often through a bare foot, but it is sustained by a shared environment. A person can be treated and still return to the same contaminated ground. A child can be blamed for being tired when the real chain runs through poor sanitation, warm moist soil, and repeated exposure. The myth individualizes the result. The evidence puts the result back inside a system.
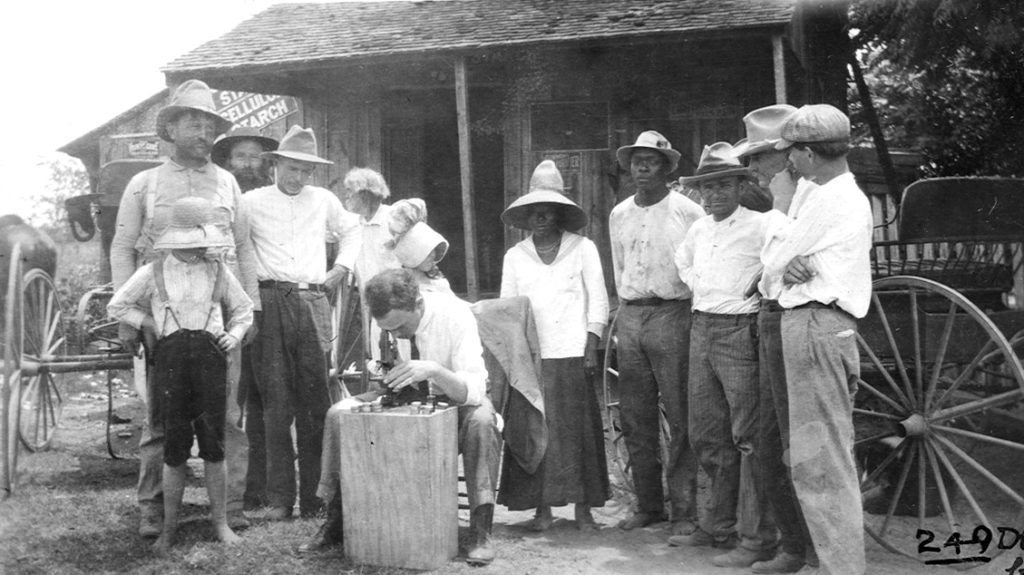
Image context: the cover photograph shows people at a Rockefeller Sanitary Commission dispensary looking through a microscope. That is not decoration. It captures the campaign's strongest educational move: making a parasite that could otherwise be dismissed as rumor or stigma visible in a local public setting.[3]
Timeline anchors
- 1902: after hookworm was discussed publicly, the "germ of laziness" language helped tie the disease to regional and class stereotypes rather than to sanitation and exposure.[3]
- 1909: John D. Rockefeller Sr. funded the Rockefeller Sanitary Commission for the Eradication of Hookworm Disease with a one-million-dollar donation, launching a five-year campaign across the South.[4][5]
- 1909-1914: the commission worked in 11 Southern states; a later historical analysis found that about 40% of the surveyed population was infected, while also warning that county selectivity limited what the campaign could prove about prevalence and eradication.[5]
- 2023: WHO still described soil-transmitted helminth infections as among the world's most common infections, with an estimated 1.5 billion people infected globally and control built around deworming, health education, and improved sanitation.[2]
Myth: hookworm made people lazy
The better wording is that heavy hookworm infection can make people sick in ways that outsiders may misread as laziness. CDC lists fatigue, abdominal pain, diarrhea, appetite loss, weight loss, and anemia among possible effects of heavier infection. In children, repeated heavy infection can slow physical and cognitive growth because adult worms attach to the intestine and feed on blood.[1] WHO puts the same mechanism into population language: infected children can become nutritionally and physically impaired, and blood loss can worsen iron-deficiency anemia in girls and women of reproductive age.[2]
That is not a personality description. It is a blood-loss and nutrition problem. The moral vocabulary did harm because it let observers treat visible tiredness as evidence about willpower. The biological vocabulary is more demanding. It asks who has contact with contaminated soil, who has shoes, who has sanitary separation of waste from human contact, who can get diagnosis and medication, and who is likely to be reinfected after treatment.[1][2]
The Rockefeller campaign understood that visibility was part of the barrier. The archive's history describes dispensaries where people could see hookworms through microscopes, get tested, receive treatment, and encounter public education in one place.[3] That does not make the campaign a simple triumph. It does show why the microscope mattered. It moved the conversation away from rumor and stigma toward a parasite that could be seen, named, and interrupted.
Myth: medicine alone solved it
Treatment was necessary, but treatment by itself was not the whole intervention. CDC's current prevention guidance still makes the sequence plain: avoid walking barefoot where hookworm is common or where human feces contaminates soil, reduce skin contact with contaminated soil, wash hands, use improved sanitation where available, and do not defecate outdoors when avoidable.[1] WHO's control framework is similarly layered: periodic deworming to remove worms, health education to prevent reinfection, and improved sanitation to reduce soil contamination.[2]
The historical Rockefeller language was rougher but recognizably similar. Its public-health explanation centered on three barriers: treat infected people so their feces no longer carried eggs, build safer privies so fecal matter did not leak into soil, and wear shoes year-round to protect feet from larvae that escaped the other measures.[3] Those measures are modest only if one ignores poverty. Shoes cost money. Privies require materials, labor, maintenance, and norms around use. Treatment requires trust, diagnosis, a supply chain, and follow-up. Hookworm was "simple" in the sense that the biological cycle was tractable; it was not simple in the social sense.
This is where the myth of a miracle cure becomes misleading. A medicine can clear worms from one body, but it cannot, on its own, keep feces out of soil or keep bare feet away from larvae. The more accurate lesson is that hookworm control needs a loop: find infection, treat it, change exposure, and keep the environment from reseeding the next case.[1][2][3]
Myth: the Rockefeller campaign proves eradication is just willpower
The Rockefeller Sanitary Commission did something real. The photo essay describes it as the first comprehensive attempt to combat hookworm in the Southern United States, and it emphasizes the campaign's role in institutionalizing services at state and local levels.[4] The effort brought physicians, schools, churches, newspapers, local leaders, and dispensaries into a coordinated campaign. It also helped make public health a practical county-level activity rather than only a distant medical idea.[4][5]
But the strongest history keeps the limits visible. Elman and coauthors argue that the commission's goals were to estimate prevalence, provide treatment, and eradicate the disease, but that the project faced resistance, limited time, limited resources, and selective county participation.[5] That matters because the campaign's archive can make the effort look smoother than it was. A county with an energetic teacher, local physicians, or receptive leaders could produce examinations and treatment quickly; another county could remain outside the effective reach of the program. The result was not a clean conquest of hookworm. It was a partial public-health buildout that exposed how much implementation depends on local institutions.[4][5]
That boundary is not a reason to dismiss the campaign. It is the reason the campaign remains useful. Hookworm made public health concrete. It showed that a disease could be mapped, demonstrated, treated, and reduced only when medical evidence met local trust, ordinary infrastructure, and repeated contact with households. It also showed how easily a program can overstate reach when the people most in need are the hardest to enroll.
What the evidence leaves us with
The hookworm story is not mainly about an old parasite in an old South. It is a durable warning about how health myths form. When disease produces fatigue, weakness, school difficulty, or reduced productivity, a society can either ask about exposure and systems or blame the person in front of it. Hookworm's evidence forces the first question.
The current global burden keeps the history from becoming quaint. WHO still frames soil-transmitted helminth infections as a disease of poor access to water, sanitation, and hygiene in tropical and subtropical areas, and it counts hundreds of millions of children and women living in areas where treatment and preventive interventions are needed.[2] CDC's prevention advice still sounds materially specific: shoes, sanitation, avoiding contaminated soil, handwashing, and safe food handling.[1] The science has changed, but the practical logic remains familiar.
So the myth fails twice. Hookworm was not laziness, and control was not a single pill. It was, and remains, a test of whether public health can keep the whole chain in view: parasite, soil, foot, intestine, blood loss, privy, shoe, school, clinic, and return visit. The microscope at the Waller County dispensary was powerful because it turned blame into evidence. The harder work was making that evidence durable enough to change the ground people walked on.[3][4][5]
Sources
- Centers for Disease Control and Prevention, "About Hookworm" - transmission, symptoms, at-risk groups, prevention, diagnosis, and treatment.
- World Health Organization, "Soil-transmitted helminth infections" - global burden, nutrition and anemia effects, and current control strategy.
- Rockefeller Archive Center, "Public Health: How the Fight Against Hookworm Helped Build a System" - campaign history, stigma language, prevention logic, and dispensary image context.
- Rockefeller Archive Center, "Photo Essay: The Rockefeller Sanitary Commission and the American South" - archival photographs and campaign summary for the Southern hookworm program.
- Cheryl Elman, Andrew S. London, and Robert A. McGuire, "Extending Public Health: The Rockefeller Sanitary Commission and Hookworm in the American South," American Journal of Public Health, 2014 - scholarly analysis of project goals, coverage, selectivity, and limits.