The modern endoscope is easy to misread because it now looks inevitable. A thin tube bends, a lens or sensor sends an image to a screen, and a clinician can inspect, biopsy, remove, cauterize, clip, dilate, or guide therapy without opening the abdomen. But the event that made that routine possible was not simply the arrival of a better camera. It was the moment a stomach instrument learned to bend without losing the image.
The decisive threshold ran from 1954 to 1961. Basil Hirschowitz, then tied to the University of Michigan gastroenterology world, read the new fiber-optics work of Harold Hopkins and Narinder Kapany, traveled to Britain to discuss the problem, and then worked with physicist C. Wilbur Peters and student Larry Curtiss to make their own workable glass fibers.[1][4] The result was not elegant at first. It was a laboratory-built route for light: hair-thin fibers, coatings, bundles, and a clinical wager that a flexible tube could show the stomach from inside without the stiffness that had defined earlier gastroscopy.
That is why this story belongs in health history rather than gadget history. The innovation changed the clinical sequence. Before flexible fiberoptics, upper gastrointestinal diagnosis often leaned on symptoms, barium X-rays, surgery, and difficult semi-rigid instruments that required skill and tolerance from both physician and patient.[4] After the fiberoptic turn, the lumen of the gut became a navigable visual space. The instrument did not merely look. It made looking repeatable.
Timeline anchors
- January 1954: Nature published fiber-optics work that showed how coated glass fibers could transmit images through flexible bundles with less light loss.[1][4]
- 1954-1956: Hirschowitz, Peters, and Curtiss worked in Ann Arbor on glass drawing, coating, and bundling because suitable commercial fibers were not available for their purpose.[1][4]
- Late 1956: Curtiss produced the glass-coated fiber quality needed for a gastroscope bundle, moving the idea from optical principle toward an instrument.[1]
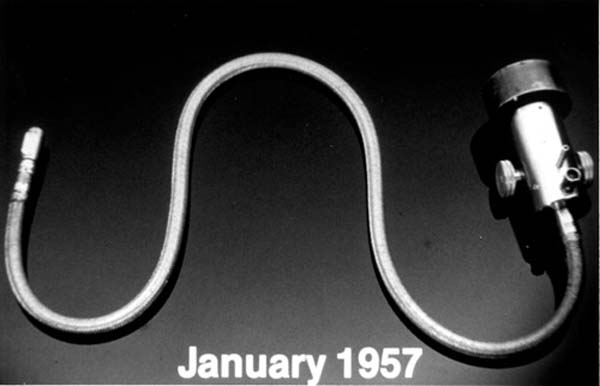
- January-February 1957: the prototype crossed into practical testing; the Dittrick Medical History Center records Hirschowitz passing it down his own throat and then using it on a patient soon after.[1][3]
- May 1957-July 1958: the team demonstrated the fiberscope publicly, and the original Gastroenterology demonstration paper appeared the following year under Hirschowitz, Curtiss, Peters, and Pollard's names.[2][4]
- October 1960: the first production model reached Hirschowitz after collaboration with American Cystoscope Manufacturing Inc.[1]
- 1961: Hirschowitz examined a patient with the fiberscope in the archival clinical photograph preserved by Dittrick, and the instrument entered the published clinical argument that conventional gastroscopy had become obsolete.[1]
The older problem was not only darkness
Endoscopy had existed long before Hirschowitz. The hard part was not the general idea of looking inside the body. The hard part was doing so deep enough, safely enough, brightly enough, and comfortably enough to become ordinary medicine rather than a specialist ordeal.
The Harvard case history describes the nineteenth-century and early twentieth-century inheritance clearly: earlier instruments used metal tubes, lenses, and lamps, then later semi-flexible gastroscopes reduced some dangers but remained difficult to use and limited in adoption.[4] They could show important things, but their shape imposed a clinical penalty. A rigid or semi-rigid instrument asks the patient's anatomy to accommodate the tool. A flexible instrument asks the tool to accommodate the route.
That distinction is the core event. The stomach is not a straight corridor. It is reached through mouth, throat, esophagus, and turns that make stiffness clinically consequential. If the instrument cannot bend while preserving a coherent image, the examiner either sees too little, causes too much discomfort, or needs a level of procedural virtuosity that keeps the method from spreading.
Glass fibers solved the wrong-looking problem first
Fiberoptics sounds abstract until the clinical problem is stated physically. Light and image had to travel along a tube that could curve. Uncoated fibers leaked light and degraded images when bent. The 1954 optical papers mattered because they made coating part of the answer: keep light guided inside the fibers so the bundle could carry an image around curves.[4]
Hirschowitz's team then had to manufacture the premise by hand. Dittrick's account says Hirschowitz and his Ann Arbor associates devised a makeshift but effective method of drawing their own glass fibers, and that Curtiss's late-1956 success produced the glass-coated fiber with the optical qualities needed for the bundle.[1] The Harvard working paper adds the texture: because no adequate commercial fibers existed for them, the team melted glass rods, drew out fibers, and experimented with coatings until a durable glass-clad solution emerged.[4]
The important point is that the breakthrough was not a single object but an alignment of material properties. The fiber had to be thin enough, coated enough, coherent enough, bundled enough, and durable enough to preserve image while bending. A small failure in any one part would turn a medical instrument into a blurry light pipe.
Self-testing made the threshold bodily
Medical invention stories often over-romanticize self-experiment, and this one does not need romance. Hirschowitz swallowing the prototype matters because it marks where optical benchwork became a bodily claim. Dittrick dates the practical crossing to February 1957, when Hirschowitz passed the first prototype down his own throat and, a few days later, down a patient's.[1]
That episode did not prove safety for all patients. It did prove something narrower and necessary: the flexible instrument could traverse the upper gastrointestinal route in a living person while still serving as an instrument of vision. In an event reconstruction, that is the line to watch. Before the self-test, the fiberscope was a promising optical device. After it, the device had entered the anatomy it was built for.
The May 1957 demonstration then translated bodily proof back into professional proof. The Harvard case history's telephone-directory detail is almost comic, but technically revealing: if observers could read print through the eyepiece, the bundle was preserving useful image information, not merely emitting light.[4] That demonstration made the device legible to clinicians who needed to believe the image before they could trust the procedure.
Manufacturing turned invention into a clinical route
The next step was production discipline. A prototype can be coaxed, protected, and explained by its makers. A clinical instrument must survive ordinary handling, patient movement, cleaning, repeated use, and the skepticism of physicians who have other ways to diagnose disease.
Dittrick records that Hirschowitz collaborated with ACMI to produce a practical instrument, receiving the first production model in October 1960.[1] ASGE's Hirschowitz lecture page identifies him as assembling the original prototype in January 1957, and the PubMed record for the original 1958 Gastroenterology report preserves the team's public demonstration of a new gastroscope called the fiberscope.[2][3] These accounts fit together: the event was neither only January's prototype nor only October 1960's model. It was the passage from prototype to manufacturable clinical object.
The early device still had limits. The Harvard working paper notes early complaints about image quality, maneuverability, safety, fragility, cost, and the lack of tissue-sampling capability in early fiber instruments.[4] That matters because it keeps the reconstruction honest. Flexible fiberoptic endoscopy did not arrive fully mature. It arrived good enough to change the design race.
The real victory was extensibility
Once the route worked, the instrument could evolve. Dittrick's artifact essay lists later refinements in the late 1960s and early 1970s: wider fields of vision, channels for biopsy forceps, suction, air, or water, and four-way controlled tip deflection.[1] It also names therapeutic milestones such as colon polypectomy in 1971, pancreatic duct cannulation in 1972, biliary stone removal in 1975, and feeding-tube placement by gastrostomy in 1979.[1]
Olympus's history page tells the same larger arc from the manufacturer side. Glassfiber endoscopes allowed direct observation of the stomach interior, then gastrocameras with fiberscopes and later endoscope designs expanded diagnosis and treatment across the esophagus, duodenum, large intestine, bronchus, and gallbladder.[5] In that telling, the key change is not just better viewing. It is a platform shift: once a flexible instrument can enter, illuminate, and show the lumen, designers can add control, recording, biopsy, suction, water, and treatment.
That is the reason the 1957 prototype should not be remembered as a curiosity. It created an extensible path. The first flexible fiberoptic endoscope did not contain the whole future of minimally invasive gastrointestinal care, but it made the future mechanically plausible.
What changed at the bedside
At the bedside, the practical change was sequence. A physician could look before cutting. A lesion could be seen in place. A suspicious area could later become a biopsy target. Bleeding, narrowing, ulceration, polyps, and duct access could increasingly become procedural problems inside the lumen rather than only external surgical problems.
Olympus describes the instrument's broader significance in those terms: glassfiber endoscopes allowed direct observation of the stomach interior, and later endoscopes widened the same route into other regions and therapeutic uses.[5] That claim should be read with historical caution. The first fiberscope was not today's therapeutic endoscope. But it changed the grammar of care. The hollow organ became a space that could be entered repeatedly, inspected dynamically, and eventually treated through the same route.
The best summary is therefore not "Hirschowitz invented the endoscope." He did not. The better claim is sharper: Hirschowitz, Peters, and Curtiss helped endoscopy cross the bendable-image threshold. Once light and image could travel around the body's curves, gastrointestinal medicine gained a new kind of access. The stomach stopped being a suspected chamber inferred from symptoms and shadows alone. It became a place that could be visited.
Sources
- Dittrick Medical History Center, Case Western Reserve University, "Hirschowitz fiberoptic Endoscope, 1960" - artifact history for the 1954-1961 development sequence, self-test, ACMI production model, and later endoscopic refinements.
- B. I. Hirschowitz, L. E. Curtiss, C. W. Peters, and H. M. Pollard, "Demonstration of a new gastroscope, the fiberscope" (Gastroenterology, 1958; PubMed record) - original demonstration-paper record for the fiberscope.
- American Society for Gastrointestinal Endoscopy, "Endowment Funds: Basil I. Hirschowitz, MD Endowed Lecture" - ASGE note identifying Hirschowitz's January 1957 original prototype flexible fiberoptic endoscope and his role in gastrointestinal endoscopy.
- Amar Bhidé, Srikant Datar, and Katherine Stebbins, "Gastrointestinal Endoscopy - Without Cutting In," Harvard Business School Working Paper 20-005 - historical case used for prior-device limitations, the 1954 fiber-optics papers, prototype development, May 1957 demonstration, and early clinical constraints.
- Olympus, "Birth of Fiberscopes," History of Olympus Products: Endoscopes - manufacturer history of glassfiber endoscopes, direct stomach observation, fiberscope gastrocameras, and the expansion of endoscopic applications.
- Optica, "Fiber-Optic Endoscope, 1957" - source page for the archival prototype photograph used as this article's image.