
BMJ Learning's Epley manoeuvre video is worth watching because it makes a common medical problem look less mysterious without making it casual. Benign paroxysmal positional vertigo, or BPPV, is often described by patients as the room spinning after rolling in bed, looking up, bending over, or changing head position. That description is frightening, but the best version of care does not begin by treating all dizziness as the same thing. It asks whether the episode is brief, positional, patterned, and compatible with a displaced inner-ear particle problem.[2][4]
That distinction is the whole point of the video. The Epley maneuver is not a generic stretch for dizziness. It is a canalith repositioning procedure: a sequence of head and body positions intended to move loose otoconia out of the posterior semicircular canal and back toward the utricle, where they stop sending the wrong motion signal.[3][5] Watch the clip with that mechanism in mind and its choreography changes character. The slow turns are not ritual. They are a physical argument about anatomy.
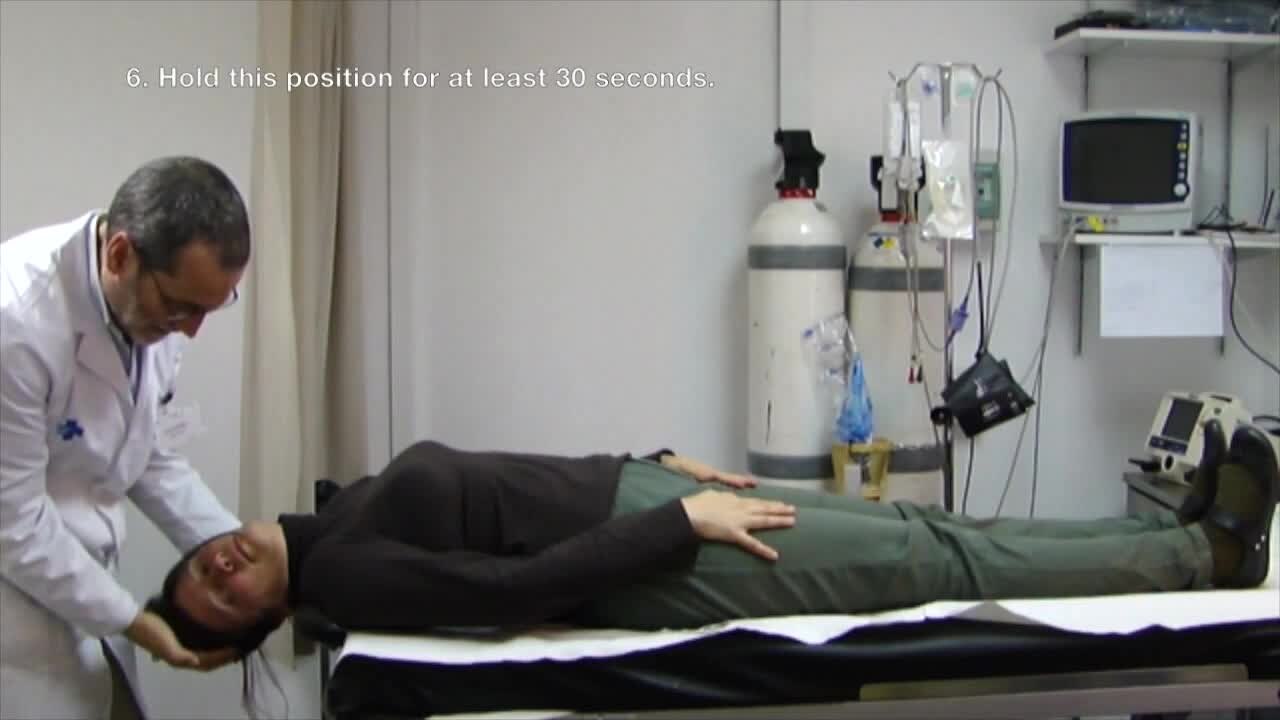
Image context: the cover image is a real clinical still from a Wikimedia Commons video of the Dix-Hallpike maneuver, sourced from an open-access clinical trial protocol. It belongs here because Epley treatment should follow a diagnosis of positional vertigo, not a guess based on the word dizziness alone.[6]
The video turns dizziness into a mechanical question
The useful thing about the BMJ Learning clip is its restraint. It does not sell the maneuver as a cure-all. It shows a patient, an examiner, a bed, and a sequence. That plainness matters because dizziness is one of medicine's messiest words. StatPearls notes that dizziness accounts for more than 3 million emergency department visits each year, while BPPV represents the most frequent peripheral vertigo cause and about 20% of patients who present with vertigo symptoms.[4] Those numbers explain the clinical temptation: if a symptom is common and unsettling, systems may over-order tests, underperform bedside exams, or reach for medication that dampens symptoms without fixing the positional cause.
The AAO-HNS guideline update pushes in the opposite direction. Its stated purpose includes improving accurate and efficient diagnosis, reducing inappropriate vestibular suppressant medication, reducing unnecessary radiographic imaging, and increasing use of appropriate therapeutic repositioning maneuvers.[2] In other words, good BPPV care is not only about knowing the Epley sequence. It is about putting the sequence in the right lane.
That lane begins with pattern recognition. Classic posterior-canal BPPV is brief and triggered by head position. StatPearls describes diagnosis as usually relying on brief episodic vertigo lasting 1 minute or less, with posterior semicircular canal BPPV diagnosed when vertigo with nystagmus occurs during the Dix-Hallpike maneuver.[4] The video should therefore be read as the treatment half of a pair: first provoke and observe the pattern safely; then reposition the particles.
The choreography is the mechanism
Around the first turn in the video, the viewer may notice how little technology is present.[1] That is the strongest visual lesson. The Epley maneuver is a bedside procedure, but it is not low-tech because it is vague. It is low-tech because the target is physical. The maneuver uses gravity and sequential orientation to move canal debris through the semicircular canal. The patient's symptoms may feel global, but the intervention is directional.[3][5]
Cochrane's review gives that bedside sequence evidentiary weight. It included 11 randomized studies with 745 participants. Five studies compared Epley against a sham maneuver, three against other repositioning maneuvers, and three against control conditions. For complete vertigo resolution, Epley was significantly more effective than sham or control; in the pooled result, resolution rose from 21% to 56%, with an odds ratio of 4.42 and a 95% confidence interval from 2.62 to 7.44.[3] Conversion from a positive to a negative Dix-Hallpike test also favored Epley over sham or control, with an odds ratio of 9.62 across eight studies and 507 participants.[3]
Those numbers are important because they keep the video from being merely persuasive. A demonstration can make a maneuver look clean even when clinical results are weak. Here the evidence supports short-term effectiveness for posterior-canal BPPV, while also keeping the boundary visible. Cochrane describes the trials as mostly small, with relatively short follow-up, and notes a high recurrence rate after treatment.[3] The lesson is not that one maneuver permanently solves every positional vertigo story. The lesson is that a correctly selected patient can often benefit from a precise physical intervention.
What the clip cannot safely imply
The video is a good anchor, but it should not be treated as a self-diagnosis license. BPPV sits inside a wider differential. StatPearls warns that central vertigo can include neurologic features such as gait disturbance, speech abnormalities, or autonomic dysfunction that may mimic BPPV, and it emphasizes differentiating benign positional vertigo from other vestibular or central causes.[4] That is the crucial safety boundary around any procedural video: the clearer the maneuver looks, the easier it is to forget that the diagnosis has to be right first.
There are body mechanics boundaries too. Cochrane found no serious adverse effects in the reviewed trials, but nausea during repositioning varied from 16.7% to 32%, and some patients could not tolerate maneuvers because of cervical spine problems.[3] That matters when reading the video. The examiner's hand support, the paced transitions, and the controlled table are not incidental. They are part of how the maneuver becomes care rather than a rough imitation of care.
The most useful way to watch, then, is to notice what is absent. The clip does not turn dizziness into a pill problem. It does not make imaging the default for a classic positional pattern. It does not encourage powering through warning signs. It makes the case that a frightening symptom can sometimes be treated by understanding the canal, the side, the sequence, and the patient's tolerance.
Why this still matters
BPPV is a small disorder only if one has never had it. A brief spinning attack can make ordinary motion feel unsafe: rolling over, showering, driving, climbing stairs, lifting a child, or getting out of bed. That is why the Epley maneuver's public-health value is larger than the simplicity of the video suggests. It converts a vague complaint into a testable, teachable, repeatable clinical pattern.
The strongest takeaway is not "try this whenever you feel dizzy." It is the opposite: do not let dizziness stay vague when the history is positional and brief, and do not let a demonstrable canal problem drift into unnecessary scans, sedating symptom control, or months of avoidance. The BMJ Learning video is useful because it shows the procedure plainly, but the evidence around it supplies the discipline: diagnose BPPV by pattern and exam, reposition when appropriate, reassess response, and step out of the BPPV script when symptoms, neurologic signs, neck limits, or recurrence demand a different plan.[2][3][4][5]
Sources
- BMJ Learning, "Vertigo - Epley manoeuvre from BMJ Learning," YouTube video.
- American Academy of Otolaryngology-Head and Neck Surgery, "Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update)" - guideline page describing diagnosis, imaging, medication, and repositioning goals.
- Cochrane, "The Epley manoeuvre for benign paroxysmal positional vertigo (BPPV)" - systematic review summary of randomized evidence for posterior-canal BPPV.
- Koshi EJ and Sutton AE, "Benign Paroxysmal Positional Vertigo," StatPearls, NCBI Bookshelf, last updated Nov. 30, 2025 - clinical overview of BPPV presentation, diagnosis, differential, and management.
- Quick M and Carr CM, "Epley Maneuver," StatPearls, NCBI Bookshelf - procedural overview of canalith repositioning for BPPV.
- Wikimedia Commons, "File:Dix-Hallpike maneuver.ogv" - clinical video still used as the article image, sourced from an open-access Trials article.