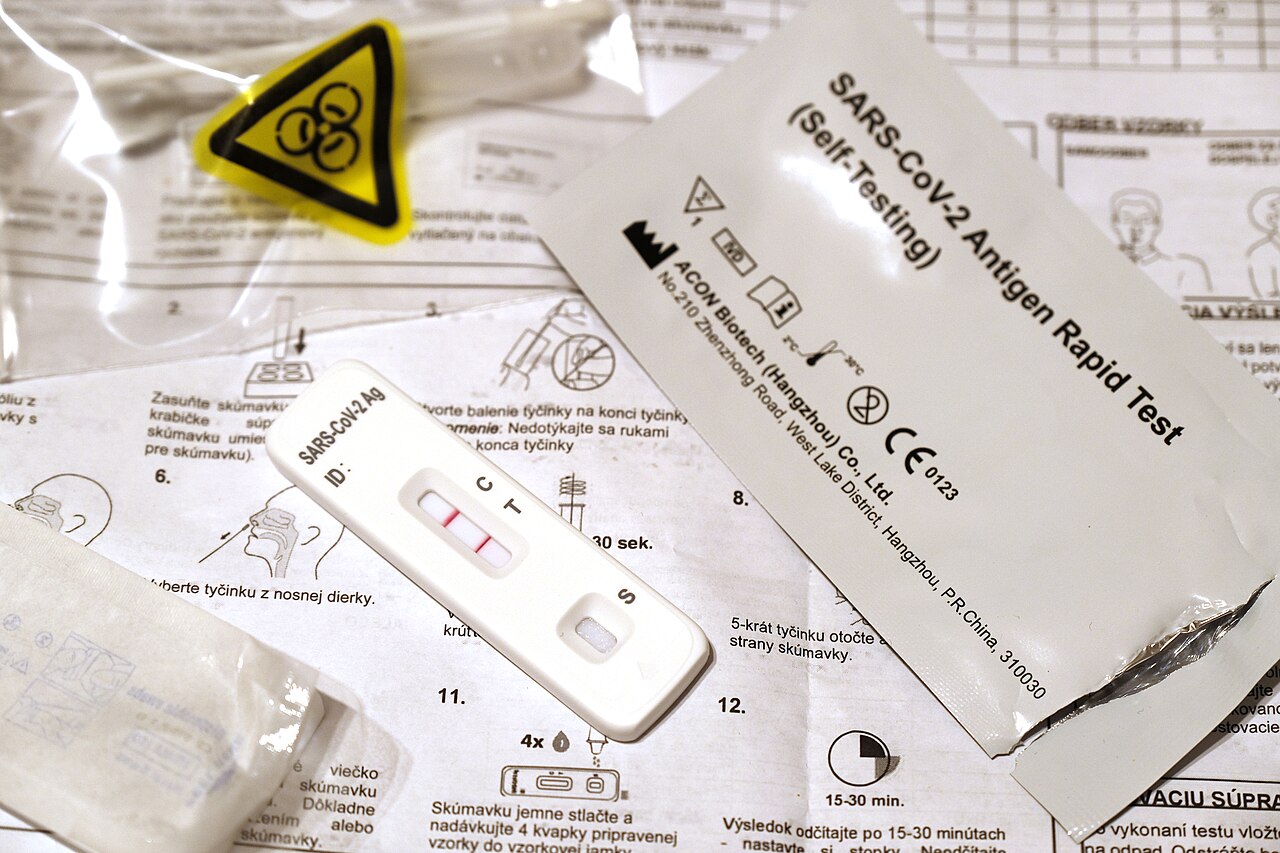

The easiest mistake with an at-home COVID-19 antigen test is to treat the cassette as a tiny court verdict. Two lines mean "case closed"; one line means "cleared"; no line means "try again later." That is emotionally understandable, because the whole promise of a rapid self-test is speed. It is also the wrong mental model. The result is not a general certificate about the next several days. It is a timed readout from one sample, taken by one person, under one set of instructions, at one point in an infection curve.
That is why CDC's short video, "How To Interpret Self-Test Results," remains useful well after the emergency phase of the pandemic. The video was made for ordinary users, not laboratory staff, and its value is that it separates three ideas that people often compress: a positive result, a negative result, and a result that should not be trusted because the test did not run correctly.[1] In July 2026, that separation still matters. CDC's current testing page, updated March 10, 2025, says antigen tests usually return results in 15 to 30 minutes, but also says a single negative antigen test cannot rule out infection.[2]
CDC's clinical overview sharpens the same point. At-home antigen tests detect viral proteins, not the viral RNA targeted by PCR and other NAATs, and they are less sensitive than most NAATs. CDC also summarizes the repeat-testing logic: negative antigen tests may need to be repeated up to three times, 48 hours apart, and negative results should be treated as a snapshot around specimen collection rather than a durable clearance document.[3] The video is worth watching with that clock in mind.
Watch the result as a fork in action, not a label
The video's first useful move is its plain categorization. A test result should create a next action. If the positive line appears, the important question is not whether the test has delivered metaphysical certainty. CDC's testing page says a positive COVID-19 test means the virus was detected and the person has, or recently had, an infection; it also says to take steps to prevent spreading COVID-19 and to seek care promptly for treatment if risk factors make severe illness more likely.[2]
That positive-result fork matters because it starts two clocks at once. The first is a prevention clock. CDC's August 18, 2025 respiratory-virus guidance says people with respiratory symptoms should stay home and away from others until symptoms are improving overall and they have been fever-free for at least 24 hours without fever-reducing medicine; after returning to normal activities, CDC recommends added precautions for the next five days, especially around people at higher risk.[4] The second is a treatment clock. CDC's February 5, 2026 treatment page says COVID-19 treatments for higher-risk people must start within five to seven days after symptoms begin, with Paxlovid and molnupiravir listed within five days and remdesivir within seven.[5]
That is the reason a positive line should not be treated as mere information. It is a routing signal. It can affect whether someone calls a clinician or pharmacist promptly, whether they avoid a dinner with an older relative, whether they work from home, and whether they wear a well-fitted mask after symptoms improve.[2][4][5] The cassette is small, but the consequence of reading it correctly is a chain of decisions.
The negative-result section needs even more discipline because a negative line feels like permission. The video is useful precisely because it refuses to let "not detected" become "not infected." CDC says a negative test means the test did not detect the virus, but it does not rule out infection; its clinical overview adds that negative results are a snapshot around specimen collection and can change if the same test is performed again later.[2][3]
The practical consequence is serial testing. If symptoms are present, CDC says FDA recommends two negative antigen tests, 48 hours apart, to be confident you do not have COVID-19. If symptoms are absent, CDC says the recommendation is three antigen tests, also 48 hours apart.[2][3] That does not make the test useless. It defines its job. A single rapid antigen test is a fast screen; a sequence of tests is a better attempt to catch a moving signal.
Early infection is the other place where the video's simplicity needs evidence context. CDC's public page says a person with symptoms may have tested before the virus was detectable, and the clinical overview says antigen sensitivity is lower than NAAT sensitivity.[2][3] That is not a bureaucratic caveat. It is biology entering the workflow. The virus may not yet be present in the sampled area at a level the test can detect. A negative result in that window should change uncertainty, not erase it.
The third fork is the invalid or errored result. This is where the control line becomes more than a visual detail. The video treats a failed test as a failed run, not as a weak negative. That distinction is easy to lose when someone is tired, sick, or trying to make a quick decision before school, work, travel, or caregiving. But the result only has meaning if the test's internal controls and manufacturer instructions are satisfied. CDC's public testing page therefore returns to the unglamorous basics: read the package insert thoroughly and follow the instructions closely.[2]
There is also something the video cannot do by itself: make the next indoor visit risk-free. CDC's testing guidance says a negative result does not rule out infection, while its respiratory-virus guidance says people may still be able to spread the virus that made them sick even after they feel better.[2][4] That line of evidence is the best antidote to over-reading the cassette. The test is one layer in a prevention stack, not a personal aerosol meter. Symptoms, exposure, local illness levels, indoor air, mask use, and the vulnerability of people nearby still matter.
Read this way, the CDC video is not just a user manual for a plastic strip. It is a small lesson in diagnostic humility. A positive result should move quickly into precautions and, for higher-risk people, treatment access. A negative result should be read against symptoms, exposure timing, and the 48-hour repeat-testing schedule. An invalid result should be repeated rather than interpreted. And no result should be asked to answer a question it cannot answer, such as whether the next indoor visit is risk-free.
The most useful habit is to decide before testing what each result will mean. If it is positive, who needs to know and what activity should be canceled? If it is negative, when is the next test and what precautions remain until the sequence is complete? If symptoms are worsening or the person is at higher risk, who can help within the treatment window? The cassette gives a line. The health value comes from making the line part of a timed plan.
Sources
- Centers for Disease Control and Prevention, "How To Interpret Self-Test Results" (YouTube video) - embedded video used for annotated viewing.
- Centers for Disease Control and Prevention, "Testing for COVID-19" (updated March 10, 2025) - current testing types, antigen-test limits, repeat-testing summary, and interpretation guidance.
- Centers for Disease Control and Prevention, "Overview of Testing for SARS-CoV-2" (updated August 29, 2024) - clinical overview of NAAT and antigen test differences, repeat testing, and snapshot limits of negative results.
- Centers for Disease Control and Prevention, "Preventing Spread of Respiratory Viruses When You're Sick" (updated August 18, 2025) - stay-home threshold and five-day added-precautions period.
- Centers for Disease Control and Prevention, "Types of COVID-19 Treatment" (updated February 5, 2026) - treatment timing, high-risk groups, and outpatient antiviral windows.
- Wikimedia Commons, "File:Positive COVID-19 rapid antigen test.jpg" - source page for the real rapid-test photograph by Marian Hubinsky.