Celiac disease is often flattened into a lifestyle sentence: gluten makes some people feel bad, so the answer is to stop eating it. The diagnostic story is stricter. Celiac disease is an immune-mediated condition in which gluten exposure can drive antibody production and small-bowel injury in genetically susceptible people. Testing works best when that reaction is still active enough to be measured. If the patient removes gluten first, the blood and tissue clues may begin to fade before anyone has documented what disease was actually present.[1][2][3]
That is why the most important word in celiac diagnosis is not "gluten-free." It is "before." NIDDK tells patients that doctors most often use blood tests and small-intestine biopsies to diagnose or rule out celiac disease, and that doctors do not recommend starting a gluten-free diet before diagnostic testing because the diet can affect test results.[3] The mechanism is simple but easy to miss: the test is not looking for a permanent identity label. It is looking for evidence of an immune process that is being sustained by gluten exposure.
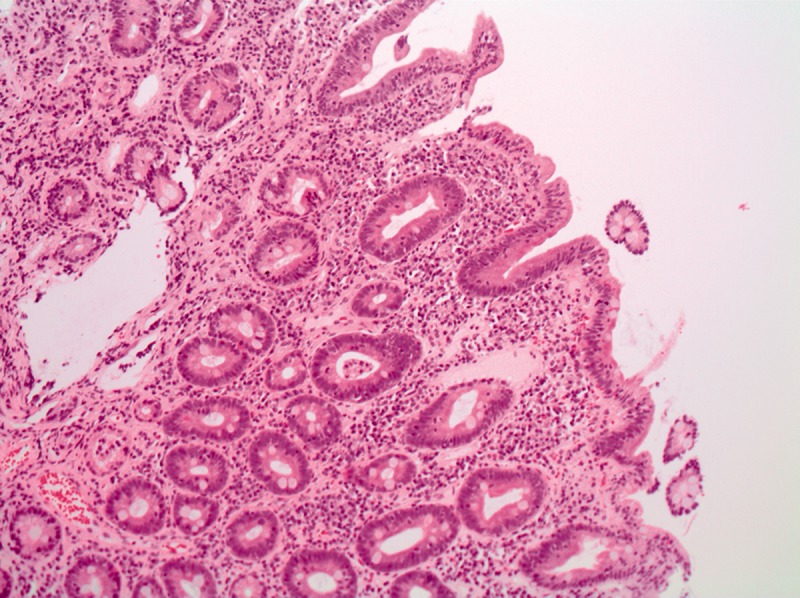
Image context: the cover image is a real microscope photograph of villous atrophy from a duodenal biopsy. It fits because celiac diagnosis is ultimately about connecting symptoms, antibodies, genetics when needed, and visible small-bowel injury rather than treating any discomfort after wheat as the same disease.[6]
Timeline anchors
- 2013: the earlier ACG guideline stated the core diagnostic principle that both serology and biopsy should be performed on a gluten-containing diet.[1]
- 2023: the updated ACG guideline kept adult diagnosis anchored in serology plus histology, with tTG-IgA measured while the patient is eating gluten and duodenal biopsy used when indicated.[1]
- 2024: a systematic review of adult no-biopsy diagnosis found that IgA-tTG at 10 times the upper limit of normal had very high specificity but only partial sensitivity, making it useful for selected patients rather than a universal shortcut.[4]
- 2026: the practical public-health lesson remains unchanged: do not make a lifelong gluten-free diagnosis by trial-and-error dieting alone when proper testing is still possible.[2][3][5]
The blood test is a live immune readout
The preferred screening test in most patients is tissue transglutaminase IgA, usually written as tTG-IgA.[2] That name sounds technical, but the logic is readable. In active celiac disease, the immune system produces antibodies associated with the gluten-driven injury process. A blood test can detect that pattern before a clinician looks directly at the intestine.
The number is not magic by itself. NIDDK summarizes the performance range for tTG-IgA as 78% to 100% sensitivity and 90% to 100% specificity, while warning that performance can depend on the degree of intestinal damage.[2] That range explains both confidence and humility. A positive result in the right clinical setting matters. A negative result does not automatically end the question when suspicion is high, when the patient has already reduced gluten, or when the immune system cannot make the usual IgA signal.
This is also why total IgA matters. NIDDK notes that 2% to 3% of people with celiac disease have IgA deficiency, compared with about 1 in 400 to 1 in 800 people in the general population.[2] If a patient is IgA deficient, an IgA-based test can be falsely reassuring. The diagnostic workflow therefore has to ask whether the measuring system is capable of hearing the signal before it decides the signal is absent.
Biopsy is not old-fashioned decoration
Blood testing narrows the target, but duodenal biopsy has a different job. NIDDK says that if serologic tests suggest celiac disease, health professionals should order upper GI endoscopy with biopsies of the duodenum, including the bulb and distal duodenum, to confirm the diagnosis.[2] The updated ACG guideline similarly keeps adult diagnosis tied to serologic and histologic data.[1]
That is not procedural stubbornness. Biopsy checks whether the disease process has reached the tissue level: villous atrophy, crypt changes, and inflammatory patterns that fit celiac disease rather than another enteropathy. It also helps when the story is discordant. A patient can have symptoms without celiac disease. A patient can have villous atrophy from another cause. A patient can have a blood result that is hard to interpret because of diet change, IgA deficiency, or pretest probability.[1][2][3]
The cover photograph makes that boundary visible. Flattened villi are not a metaphor for feeling unwell after pasta. They are tissue evidence. A serious diagnosis should preserve that distinction because the treatment is lifelong, socially burdensome, and clinically consequential.
The no-biopsy debate is a boundary test, not a permission slip
The strongest challenge to routine biopsy comes from very high antibody levels. A 2024 systematic review and meta-analysis of adults examined IgA-tTG at 10 times the upper limit of normal against duodenal biopsy. It included 18 studies and 12,103 participants from 15 countries. The result was revealing: summary specificity was 100% with a 95% confidence interval of 98% to 100%, but summary sensitivity was 51% with a 95% confidence interval of 42% to 60%.[4]
That combination matters. Very high tTG-IgA can be a powerful rule-in signal in selected adults with a moderate to high pretest probability. It is not a general rule-out tool. Most patients with celiac disease will not necessarily sit above that very high threshold, and many diagnostic settings still need histology. The no-biopsy discussion therefore sharpens the article's main claim rather than weakening it: celiac testing works only when the test, the patient, the gluten exposure, and the clinical probability are matched correctly.[1][2][4]
Gluten-free treatment can erase diagnostic evidence
The gluten-free diet is the treatment, but it is also a diagnostic spoiler when started too early. NIDDK's treatment guidance states that consuming gluten triggers an abnormal immune reaction that damages the small intestine, and that following a gluten-free diet will heal small-intestine damage for most people.[5] That is good medicine after diagnosis. Before diagnosis, it can turn the lights down on the very process clinicians are trying to observe.
The practical mistake is understandable. A person feels better after removing wheat, barley, or rye and assumes the case is solved. But symptom response is not specific enough. Irritable bowel syndrome, wheat allergy, non-celiac gluten sensitivity, lactose intolerance, medication effects, infection, inflammatory bowel disease, and ordinary dietary pattern changes can all confuse the story. Celiac disease has a particular immune and tissue signature. Losing the chance to document it can leave the patient with a demanding diet but no solid record for family screening, nutritional follow-up, bone-health assessment, or future clinical decisions.[2][3][5]
Genetics can help in selected uncertain cases, but it is mostly a rule-out tool. NIDDK notes that people with celiac disease almost always carry HLA-DQ2.5 or HLA-DQ8, yet about 30% of the general population has one of those variants and only about 3% of people with them develop celiac disease.[2] A negative result can make celiac disease very unlikely; a positive result does not prove the disease.
The clean lesson is narrow. Celiac testing is not a generic wellness screen for gluten discomfort. It is a timed attempt to catch an active immune-enteropathy chain: gluten exposure, antibody signal, IgA context, tissue injury, and clinical fit. Once that chain is documented, a gluten-free diet becomes treatment. Before it is documented, the same diet can make the diagnosis harder to prove.
Sources
- Rubio-Tapia A, Hill ID, Semrad C, et al., "American College of Gastroenterology Guidelines Update: Diagnosis and Management of Celiac Disease" (American Journal of Gastroenterology, 2023; PubMed record).
- National Institute of Diabetes and Digestive and Kidney Diseases, "Celiac Disease Tests" - professional guidance on tTG-IgA, total IgA, intestinal biopsy, genetic testing, and gluten-containing diet requirements.
- National Institute of Diabetes and Digestive and Kidney Diseases, "Diagnosis of Celiac Disease" - patient guidance on blood tests, small-intestine biopsies, and avoiding a gluten-free diet before testing.
- Shiha MG, Nandi N, Raju S, et al., "Accuracy of the No-Biopsy Approach for the Diagnosis of Celiac Disease in Adults: A Systematic Review and Meta-Analysis" (Gastroenterology, 2024; PubMed record).
- National Institute of Diabetes and Digestive and Kidney Diseases, "Treatment for Celiac Disease" - gluten-free diet treatment, healing of small-intestine damage, hidden gluten sources, follow-up, and refractory-disease boundaries.
- Wikimedia Commons, "File:Villous atrophy duodenum.jpg" - real histology photograph of a duodenal biopsy showing villous atrophy.