Rubber gloves are easy to misremember because modern medicine makes them look inevitable. They feel like part of the room itself, as basic as a scalpel tray or a sterilized gown. The historical sequence was stranger and more contingent. Gloves did not first enter Johns Hopkins as a grand antiseptic doctrine. They entered because Caroline Hampton, the chief operating-room nurse under William Halsted, could no longer tolerate what antiseptic surgery was doing to her hands.[1][2]
That distinction matters because it changes what kind of medical breakthrough this really was. The origin story is not that one brilliant surgeon suddenly deduced the universal need for barrier protection. The origin story is that an unusually efficient nurse developed severe dermatitis from the very chemicals meant to make surgery safer; Halsted tried to keep her in the room; a local fix worked; then Joseph Bloodgood supplied the harder proof by showing that gloved surgery slashed postoperative infections.[1][2][3] In other words, the rubber glove became standard only after three layers locked together: occupational injury, workflow adoption, and outcome data.
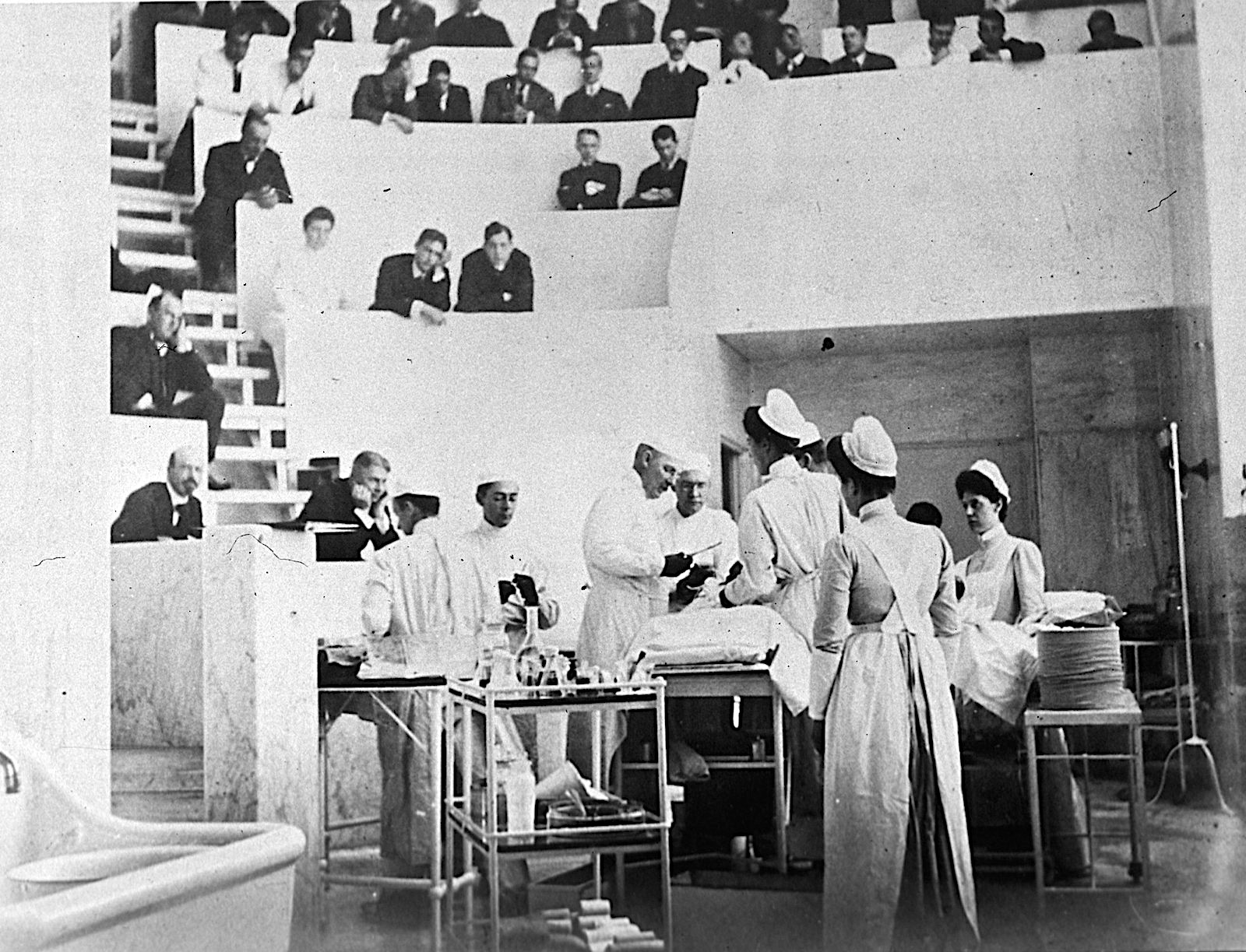
Image context: the cover image shows William Halsted and colleagues in surgery at Johns Hopkins Hospital. It belongs here because the key unit in this story is the operating room as a coordinated environment. Gloves changed what happened inside that room for nurses first, assistants next, and finally for patients whose infection risk fell once the habit became routine.[2]
Timeline anchors
- 1889: Caroline Hampton moved to Johns Hopkins Hospital and became chief nurse of the operating room under William Halsted.[1][2]
- Winter 1889-1890: repeated exposure to mercuric chloride, carbolic acid, and other disinfecting steps caused severe dermatitis in Hampton's hands and arms.[1][2]
- 1890: Halsted arranged for the Goodyear Rubber Company to make thin rubber gloves with gauntlets for Hampton; the gloves quickly spread to assistants and nurses around her.[1][2][3]
- 1893-1899: Joseph Bloodgood began wearing gloves in hernia operations and later published the infection results that made the practice harder to dismiss.[1][2][3]
- 1911: Science History Institute's summary notes that roughly half of surgeons were wearing gloves by then, a sign that the workaround had become infrastructure.[2]
The first problem was not germs in the abstract but a nurse who could no longer work
Caroline Hampton was not a decorative figure in someone else's story. The 2010 Baylor microhistory describes her as Johns Hopkins's chief operating-room nurse, valued precisely for manual dexterity and steadiness under pressure.[1] That detail is central. Gloves entered surgery through the loss-risk attached to one highly skilled worker. If Hampton left, Halsted would lose someone he considered unusually efficient in a room where efficiency was not ornamental but operational.[1]
The injury itself came from the antiseptic regime. By the late 1880s Halsted had embraced Listerian cleanliness with real zeal, and the room demanded repeated chemical exposure: soap, potassium permanganate, oxalic acid, then mercuric chloride.[2][4] Those solutions attacked bacteria, but they also attacked skin. Hampton developed severe dermatitis because her hands and forearms kept absorbing the price of the room's new purity standard.[1][2]
That is the first useful correction to the usual legend. The origin of surgical gloves is not only a story about protecting patients from clinicians. It is also a story about protecting clinicians, especially nurses, from the chemistry of early antisepsis. Before the glove became a barrier against contamination, it was a barrier against the room itself.[1][2][3]
Halsted's move was a retention fix before it was a hygiene theory
Halsted did not solve Hampton's problem with a policy memo. He commissioned equipment. The Baylor article preserves the classic account: after Hampton complained that mercuric chloride had produced dermatitis, Halsted asked the Goodyear Rubber Company to make thin rubber gloves with gauntlets as an experiment.[1] Science History Institute's retelling adds the concrete room logic around that decision: thick earlier medical gloves existed, but they were too clumsy for precise surgical work, so what mattered in 1890 was not simply using gloves, but getting a version thin enough to preserve dexterity.[2]
That emphasis on thinness matters. If the gloves had protected Hampton while ruining everyone else's touch, they would have remained a niche accommodation. Instead, they turned out to be workable. Hampton's hands improved, and the design was good enough that other nurses and assistants began adopting gloves as well.[1][2] The habit spread through imitation before it spread through doctrine.
This is why the article belongs in biography/microhistory rather than in a generic infection-control timeline. The decisive early mechanism was personal and local. One room had a staffing problem. One solution preserved the labor that made the room run. That solution then proved compatible with the tactile demands of surgery. The idea moved because it helped the team function, not because the profession had already accepted every later principle of barrier protection.[1][2][4]
Bloodgood turned a room workaround into patient-safety evidence
The story becomes harder, and more consequential, once Joseph Bloodgood enters it. According to the Baylor article, Bloodgood started using gloves himself in 1896 and later published results from more than 450 hernia operations showing a near-total collapse in infection rates.[1] Science History Institute gives the statistics in a sharper, more memorable split: in 220 hernia operations done without gloves, 38 patients developed infections, more than 17%; in 226 gloved operations, only 4 became infected, under 2%.[2] The 2024 glove-history review compresses the same transition into one line: glove use pushed postsurgical infections from above 17% down to about 2%.[3]
Those numbers are the hinge of the whole episode. They converted gloves from an occupational-protection device into a patient-outcome technology. Before Bloodgood, a skeptical surgeon could say the gloves were useful for Hampton's skin but optional for real operators. After Bloodgood, that position became harder to maintain. A surgeon could still complain about touch, but now the complaint had to stand against infection arithmetic.[1][2][3]
This is the second useful correction to the popular anecdote. Halsted did not single-handedly discover the full meaning of the glove at the first moment of invention. The deeper clinical significance emerged when Bloodgood linked glove use to postoperative outcomes in a form other surgeons could not casually wave away.[1][3] Hampton created the opening; Bloodgood supplied the conversion rate from workaround to standard.
Resistance lasted because surgeons feared numb fingers more than invisible bacteria
The fact that glove adoption still lagged tells us what surgery valued at the time. Science History Institute's account is especially good on this point: many surgeons thought touch was their supreme guide inside the body, and they feared rubber would blunt that sense at the worst possible moment.[2] The 2024 review says much the same in more formal language. Detractors believed any infection benefit might be outweighed by the loss of tactile precision.[3]
This resistance was not wholly irrational. In an era before antibiotics and before the modern abundance of imaging and perioperative support, surgery depended heavily on fingers. Tissue planes, tumor boundaries, and hidden structures were often recognized by feel. A glove that made the hand clumsy would not have looked like a minor inconvenience. It would have looked like an assault on judgment itself.[2][3][4]
What changed the balance was that thinner gloves proved more tolerable than critics predicted, while the infection signal proved larger than many surgeons wanted to admit. Gloves reduced sensation somewhat, but they also improved grip in wet conditions and, more importantly, reduced the frequency with which an operation's technical success was undone by sepsis afterward.[2][3] The profession did not convert because it suddenly loved barriers. It converted because the tradeoff shifted.
Why this microhistory still matters in 2026
The durable lesson is that some medical standards are born twice. First they appear as narrow solutions to local friction. Then they survive only if someone shows that the local fix also changes outcomes. Rubber gloves followed exactly that route. Hampton's dermatitis created the immediate problem. Halsted's custom gloves solved the labor problem. Bloodgood's infection numbers made the practice legible as a patient-safety system.[1][2][3]
That sequence still reads clearly because it is how many durable health interventions actually spread. They do not arrive as perfect abstractions. They begin as awkward accommodations inside real workplaces, then become non-negotiable only after they prove they protect both workers and patients better than the old habit did. In the glove story, the room learned first and the profession learned later.
Seen this way, Caroline Hampton belongs at the center of the history rather than at its edge. The operating room did not become safer because one famous surgeon had a clean idea. It became safer because a nurse's damaged hands exposed a weakness in early antiseptic practice, and because the fix for that weakness turned out to change the fate of patients after the incision closed.[1][2][3][4]
Sources
- S. Robert Lathan, "Caroline Hampton Halsted: the first to use rubber gloves in the operating room" (Baylor University Medical Center Proceedings, 2010) — the Hampton-Halsted timeline, the dermatitis sequence, Halsted's Goodyear order, and Bloodgood's later infection results.
- Sam Kean, "The Nurse Who Introduced Gloves to the Operating Room" (Science History Institute, 2020) — narrative reconstruction of Hampton's role, the Johns Hopkins chemical routine, the 220/38 versus 226/4 infection split, and the broader adoption arc.
- Valentina Ordoñez-Santibañez et al., "Gloving in medicine: a boon for infection prevention or a hindrance?" (Infection Control & Hospital Epidemiology, 2024) — concise historical overview of glove adoption, Bloodgood's infection evidence, and the tactile-resistance argument.
- John L. Cameron, "William Stewart Halsted. Our surgical heritage" (Annals of Surgery, 1997) — Halsted's broader surgical setting, his Listerian commitments, and the institutional context at Johns Hopkins.