The blue-baby operation became famous because color changed in the operating room. A cyanotic child, starved of enough oxygenated blood, could move from blue toward pink once a new route sent more blood to the lungs. That visible transformation made the procedure feel like a miracle. The more useful reconstruction is stricter: the first operation did not repair a malformed heart. It altered circulation around the defect.[1][2]
That distinction keeps the history honest. In November 1944 at Johns Hopkins, Alfred Blalock, Helen Taussig, Vivien Thomas, and the operating team were not yet doing the kind of intracardiac repair later pediatric heart surgery would make possible. They were building a palliative shunt, a detour between vessels, for children whose pulmonary blood flow was too limited to sustain ordinary life.[1][2][3] The operation mattered because it proved that a congenital cardiac problem could be approached by deliberately changing vascular physiology.
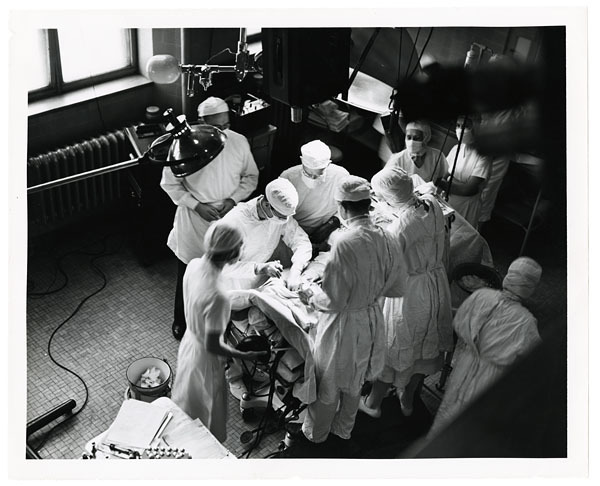
The cover image is a real 1947 archival photograph from the Johns Hopkins blue-baby exhibit. In it, the operating room looks crowded because the work was crowded: Blalock at the table, Thomas standing behind him in the technical position the published record long failed to honor, and a surrounding system of diagnosis, anesthesia, surgical assistance, and postoperative care.[3][6]
Timeline anchors before the room
- 1930: Helen Taussig was appointed to head a Johns Hopkins clinic that soon focused on congenital heart disease, putting her in daily contact with children whose cyanosis reflected too little blood reaching the lungs.[4]
- 1941: Blalock returned to Johns Hopkins as surgeon-in-chief and insisted that Vivien Thomas come with him from Vanderbilt, even though Thomas could not join the professional staff under the hospital's racial rules.[3]
- 1943: Taussig later recalled the crucial idea in a conversation about vascular bypass: if one artery could be redirected in another disease, then perhaps the subclavian artery could be connected to the pulmonary artery for blue babies.[4]
- November 1944: the first human blue-baby operation was performed on Eileen Saxon at Johns Hopkins.[2][5]
- May 19, 1945: Blalock and Taussig published the first three operations in JAMA, reporting that there had previously been no satisfactory treatment for pulmonary stenosis or pulmonary atresia.[1]
- By the end of the 1940s: the Blalock-Taussig-Thomas shunt had been performed on nearly 900 children, according to the American Heart Association's historical account.[5]
Taussig's insight was anatomical and practical
The clinical problem was not simply that these children had weak hearts. Taussig understood that many were blue because too little blood was getting to the lungs to pick up oxygen.[4][5] She had learned the physiology through a difficult clinical practice: examining children, following their decline, using available imaging and cardiac evaluation, and studying the anatomy of hearts that had failed.[4][5]
Her proposal was therefore practical rather than decorative. If a child could not send enough blood through the normal pulmonary route, perhaps surgery could create another route. The shunt idea did not promise a normal heart. It promised more lung-bound flow.[2][4]
That is why the later name matters. "Blalock-Taussig" preserves the surgeon and pediatric cardiologist, but it misses the full mechanism of invention. Johns Hopkins' own exhibit now uses "Blalock-Taussig-Thomas Shunt," a naming choice that better fits the evidence.[2][3] Taussig supplied the patient problem and circulatory hypothesis. Thomas turned the hypothesis into an operation that could be rehearsed. Blalock carried the authority and operative responsibility in the hospital theatre.
Thomas made the operation teachable before it was public
Thomas's role was not a minor assisting detail. At Vanderbilt and then Hopkins, he had already become central to Blalock's experimental surgery. For the blue-baby problem, he had to reproduce the relevant circulatory problem in laboratory dogs, test the surgical pathway, refine the sequence, and adapt tools to vessels far smaller than the adult surgical field was used to handling.[2][3][5]
The Lasker Foundation's account notes that Thomas designed a clamp for the first operation and modified needles for tiny vessels.[5] Johns Hopkins' exhibit states the broader point: Thomas created many of his own tools and perfected the technique during two years of practice on laboratory dogs.[2] That preparation changed the status of the first human operation. It was not blind bravery. It was a translation from a laboratory procedure into a fragile child, with all the moral tension that animal experimentation and surgical novelty carried.[2][7]
The first operating-room scene makes that dependency visible. Thomas stood behind Blalock on a stepstool and guided him through the technique.[2][3] Resident surgeon William Longmire later remembered that modern vascular instruments were lacking and that Thomas offered practical suggestions during the procedure.[2] The operating hierarchy put Blalock at the table and in the publication line. The technical memory of the room kept pointing back to Thomas.
Eileen Saxon's case proved possibility, not cure
Eileen Saxon survived the first operation, and the immediate color change showed that the shunt could improve oxygenation.[2][5] But she became cyanotic again within weeks and died after a second operation.[2] That outcome is central to the reconstruction. If the episode is told only as miracle, the boundary disappears. The first case showed that the physiology could be changed; it did not show that the operation was safe, durable, or curative for every child.
The next two cases made the evidence stronger. In the 1945 JAMA report, Blalock and Taussig described three children treated over the previous three months, emphasizing that children with pulmonary stenosis or pulmonary atresia had previously been beyond useful surgical help.[1] The abstract states that the second and third patients had deep persistent cyanosis that greatly diminished or disappeared, with proportional improvement in general condition.[1]
Those were early results, cautiously written by modern standards but explosive in their moment. They shifted congenital heart disease from a domain of diagnosis and hospice-like expectation into a domain where anatomy could invite intervention. The shunt was temporary and incomplete, but it opened the operating room door.
The operation reorganized pediatric heart disease
The later numbers show how quickly a local experiment became a destination system. The American Heart Association account says nearly 900 children received the procedure by the end of the 1940s alone.[5] Families traveled to Hopkins because the operation gave a previously unreachable group of children a chance at more time, better color, and more activity.[3][5]
It also changed the training ecology around Hopkins. Taussig's clinic diagnosed and followed the children. Blalock's surgical service drew physicians who wanted to learn the new procedure. Thomas trained generations of surgeons in surgical technique even while formal credit lagged behind his contribution.[3][4] The work therefore created not only a procedure, but a school of practice.
The procedure's limits shaped its legacy. It was a shunt, not a complete anatomical repair. Many children needed later operations, and modern congenital heart surgery often uses different definitive repairs for the same underlying conditions.[5] Yet the principle remained powerful: if a child's circulation is failing because flow is routed badly, surgery can sometimes redraw the route before it can rebuild the whole heart.
What the reconstruction preserves
The blue-baby operation is most useful when read as a chain rather than a legend. Taussig recognized that the visible blue color traced back to pulmonary blood-flow failure. Thomas converted that insight into a repeatable vascular technique, with instruments and practice scaled to tiny anatomy. Blalock carried the procedure into the operating room and accepted the risk of the first human cases. Anesthetists, residents, nurses, and postoperative teams then had to keep the child alive long enough for the new route to matter.[2][3][4][5]
That chain also explains the injustice in the older credit structure. The 1945 paper lists Blalock and Taussig, not Thomas.[1][3] The omission reflected the racial and professional order of the hospital as much as the mechanics of discovery. Johns Hopkins later recognized Thomas with an instructor appointment and an honorary degree in 1976, but the delayed honor does not erase the earlier asymmetry.[3]
The clinical lesson remains separate from the moral one, but they strengthen each other. Medical breakthroughs often appear as sudden operations because the public sees the moment when the body changes. The blue-baby operation shows the quieter machinery underneath: a diagnostic pattern, a physiologic hypothesis, laboratory rehearsal, toolmaking, institutional hierarchy, and a team ready to act before certainty was complete. The child turning pink was the visible sign. The deeper breakthrough was that congenital heart disease had become surgically thinkable.
Sources
- Alfred Blalock and Helen B. Taussig, "The Surgical Treatment of Malformations of the Heart: In Which There Is Pulmonary Stenosis or Pulmonary Atresia," JAMA 128(3), 1945 - PDF copy of the first report on the three operations.
- Johns Hopkins Sheridan Libraries, "The Blalock-Taussig-Thomas Shunt" - exhibit page describing Taussig's shunt idea, Thomas's laboratory technique, Eileen Saxon's operation, and the 1945 publication.
- Johns Hopkins Sheridan Libraries, "Vivien Thomas" - exhibit page documenting Thomas's laboratory role, his position behind Blalock in the operating room, delayed credit, and later recognition.
- Johns Hopkins Sheridan Libraries, "Helen Taussig" - exhibit page on Taussig's congenital-heart clinic, the pulmonary blood-flow insight, the 1943 bypass idea, and her role in diagnosis and postoperative care.
- Lasker Foundation, "Making Mothers and Children Healthier" - historical account of Eileen Saxon's operation, Thomas's instruments and technical role, the 1954 Lasker Award, and the shunt's later pediatric use.
- Johns Hopkins Sheridan Libraries, "Vivien Thomas" image source - archival 1947 overhead photograph of a blue-baby operation used as the article cover.
- Johns Hopkins Sheridan Libraries, "Anna the Dog" - exhibit page on the laboratory dog whose survival helped validate the experimental procedure before the first human operation.