Phossy jaw is easy to misremember as a Victorian horror story about bad matches. The stronger health lesson is more precise. White phosphorus made strike-anywhere matches convenient, cheap, and profitable, but it also moved a toxic production material into the mouths, teeth, gums, and bones of workers who handled the paste every day.[1][2]
The disease was not solved by a heroic surgical breakthrough. It was solved when prevention moved upstream: substitute safer match chemistry, remove white phosphorus from the manufacturing process, inspect factories, and make continued use economically and legally unattractive.[2][3][4] In public-health terms, phossy jaw is a case where the cure was not better rescue after exposure. The cure was redesigning the exposure out of the job.
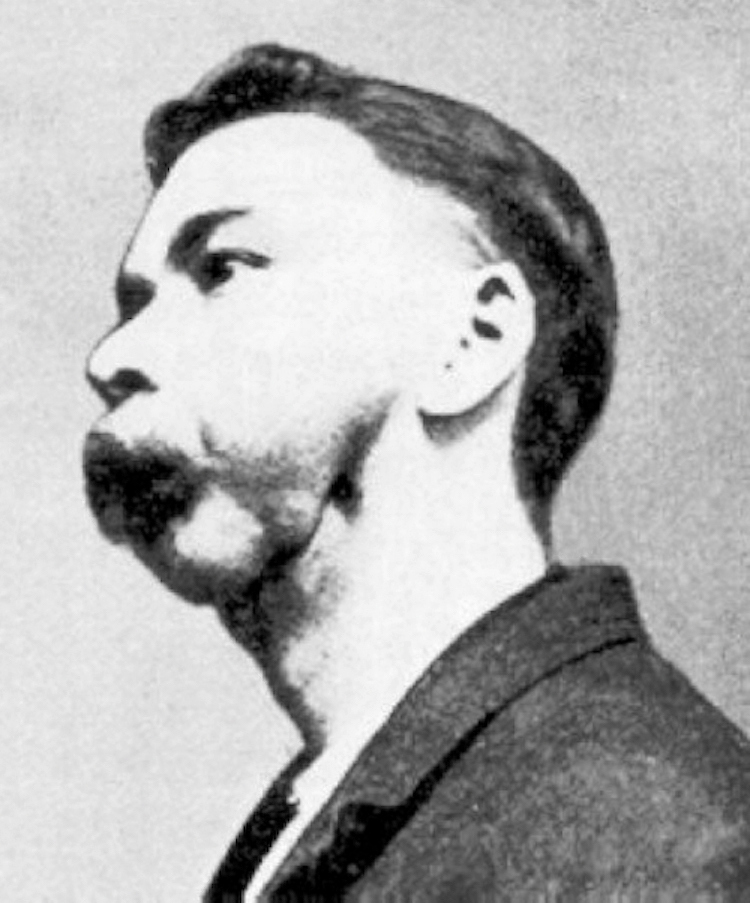
Image context: the cover uses a real 1899 photograph of a match factory worker with phossy jaw, described by Wikimedia Commons as showing pathological fracture of the mandible and fistula formation.[6] It belongs here because the article is about the bodily endpoint of a manufacturing choice. The injury was not symbolic. It was tissue, bone, infection, and work history made visible.
The useful match created the exposure route
White phosphorus entered match production because it made ignition easier. The Royal College of Surgeons describes the early nineteenth-century shift plainly: adding yellow, now called white, phosphorus to match heads helped create the profitable "strike-anywhere" match industry.[2] That small convenience mattered commercially. A match that lights readily is a better consumer product.
The same property made the factory dangerous. Workers were not merely near a sealed chemical. They mixed, dipped, packed, and handled phosphorus-containing material in rooms where particles and vapors could contaminate faces, fingers, clothing, teeth, and oral tissues.[1][2][5] The historical review in the British Dental Journal notes that the first clinical sign often appeared in the mouth as a localized dull red mucosa, then ulceration and chronic infection.[1] That sequence matters because it keeps the mechanism local and occupational: the jaw was not randomly chosen by fate. The route ran through the mouth.
By 1858, detailed medical reports of jaw-bone disease in match workers were appearing.[2] The Royal College of Surgeons recounts an even earlier New York case: Cornelia, a 16-year-old match-factory worker, developed toothache and swelling in 1855, then underwent removal of dead jaw bone in 1856.[2] Those dates show that the disease was not an obscure late discovery. The medical profession had warning signals decades before the major legislative closures.
The injury was bone death plus infection
The phrase "phossy jaw" can sound almost folkloric, but the clinical process was brutal. The historical review describes the major feature as a loss of bone vitality followed by chronic osteomyelitis, with ulceration, chronic infection, and sequestra: pieces of dead bone separating from living bone.[1] In the older reports, those sequestra were irregular, porous, and heavily resorbed.[1]
That mechanism explains why ordinary dental care could miss the true cause. A worker might first present with toothache, swollen gums, abscesses, or a draining opening. Those symptoms could be treated as local dental trouble unless someone connected them back to the factory material.[2] Public health had to make the chain visible: phosphorus exposure at work, oral contamination, mucosal injury, bone death, infection, disfigurement, disability, and sometimes death.
This also explains why the disease belonged so strongly to poverty and labor conditions. The Royal College of Surgeons calls it overwhelmingly a disease of the poor and notes that many victims in nineteenth-century case histories were young adults who had worked in the industry since childhood.[2] A safer chemistry existed, but cost and competition slowed the switch.[2][3] The hazard persisted because the people absorbing it were workers with weak bargaining power, not because the body was mysterious.
Treatment could not solve the production problem
Surgery could sometimes remove dead bone. The 1856 Cornelia case shows how dramatic that could become: diseased jaw was removed in stages, under conditions far from modern maxillofacial surgery.[2] But successful removal of necrotic bone did not make the workplace safe for the next worker. It only treated one body after the exposure had already done its damage.
The stronger intervention was substitution. The CDC Stacks record for McGlothlin and Myers's 1996 review says the availability of sesquisulfide as a safer alternative helped eradicate production of phosphorus-containing matches and the associated necrosis.[3] The Royal College of Surgeons similarly notes that the disease could be prevented by using safer red phosphorus and occupational hygiene.[2] The lesson is not subtle: once the hazardous input was no longer necessary for match production, continued use became a policy and market failure.
This is why phossy jaw is best read as a causal mechanism rather than as a morality tale. The mechanism had four linked parts:
- A product requirement: matches should ignite readily.
- A hazardous manufacturing solution: white phosphorus paste.
- A worker exposure route: oral and facial contamination during production.
- A prevention route: replace the chemical and enforce the replacement.[1][2][3]
If any account dwells only on gruesome symptoms, it misses the public-health hinge. Phossy jaw became preventable when the match itself was redesigned.
Law had to neutralize the cheap-danger advantage
The hardest policy problem was competition. A factory that kept using white phosphorus could make the familiar product cheaply while safer producers carried higher costs. That is why the disease could not be solved by individual virtue alone. A single benevolent factory could reduce harm locally and still be undercut by manufacturers that kept the dangerous process.
International and national rules attacked that advantage. The Royal College of Surgeons places the international prohibition point at the 1906 Berne Convention, followed by national bans over the next few years.[2] In Britain, the White Phosphorus Matches Prohibition Act took official form in 1908; the enacted text prohibited the manufacture, sale, and importation of matches made with white phosphorus after the transition dates it set.[4] In the United States, the CDC Stacks summary points to the 1912 Match Act, which used a prohibitive tax on each box of matches made with white phosphorus and paired that with inspection and testing capacity.[3]
Those mechanics matter. The intervention was not only "ban the bad thing." It was a package: safer substitute, tax pressure, factory inspection, chemical differentiation, and international coordination.[3][4] That package changed the incentive structure around the match head. Once the cheaper hazard lost its market advantage, occupational disease prevention could finally beat production convenience.
The modern echo is not identical, but it is useful
Modern articles sometimes connect phossy jaw to medication-related osteonecrosis of the jaw, especially because both involve jaw-bone necrosis and have been discussed through phosphorus-related chemistry.[1][5] That comparison can be useful, but it should not blur the historical mechanism. Nineteenth-century phossy jaw was an occupational exposure disease rooted in manufacturing conditions. Medication-related jaw osteonecrosis belongs to a different clinical and risk-benefit setting.[1][5]
The better modern lesson is about prevention hierarchy. When a hazard is built into a process, personal caution and late treatment sit too low in the chain. Workers can be told to be careful. Doctors can learn to recognize symptoms. Surgeons can remove damaged tissue. All of that may matter, but none of it is as strong as eliminating the exposure from the process that keeps generating cases.
That is why phossy jaw deserves a place in health history even after the match industry changed. It shows an occupational disease moving from case reports to causal recognition to substitution to law. The dates mark the slow climb: clinical recognition by the mid-nineteenth century, labor and reform pressure in the late nineteenth century, Berne in 1906, British prohibition in 1908, and the U.S. Match Act in 1912.[2][3][4]
The disease ended not because jaws became easier to repair, but because white phosphorus matches stopped being the normal way to make fire. Public health won when it moved the question from the patient's mouth to the factory formula.
Sources
- Hugh Devlin, "A historical review of 'phossy jaw'," British Dental Journal, 2023 - clinical mechanism, oral entry pathway, chronic osteomyelitis, sequestra, and comparison boundaries.
- Royal College of Surgeons of England, Susan Isaac, "'Phossy jaw' and the matchgirls: a nineteenth-century industrial disease" (September 28, 2018) - match chemistry, nineteenth-century cases, Cornelia's surgery, reform pressure, and prevention through safer phosphorus.
- CDC Stacks / NIOSH record for James D. McGlothlin and Melvin L. Myers, "Matchmakers' 'phossy jaw' eradicated," American Industrial Hygiene Association Journal, 1996 - eradication, sesquisulfide substitution, 1912 Match Act, inspections, and testing.
- legislation.gov.uk, "White Phosphorus Matches Prohibition Act 1908" - enacted British statute prohibiting manufacture, sale, and importation of white-phosphorus matches after transition dates.
- R. A. Pollock et al., "'Phossy Jaw' and 'Bis-phossy Jaw' of the 19th and the 21st Centuries," Craniomaxillofacial Trauma & Reconstruction, 2015 - historical white-phosphorus exposure context and modern comparison boundary.
- Wikimedia Commons, "File:Match factory worker with phossy jaw.jpg" - 1899 archival clinical photograph used as the article image.